FORWARD HEAD POSTURE (FHP), ALSO DEscribed as cervical anterior translation, is one of the most common postural distortions seen in modern practice.
When the head sits forward of the thorax, joint mechanics change, cervical extensor demand rises, and afferent input from cervical mechanoreceptors is altered, influencing sensorimotor control.1 Clinically, chiropractors often observe FHP as part of broader kinetic-chain patterns that link cranial position with thoracic and pelvic alignment.2
Persistent anterior translation has been associated with neck pain, reduced cervical range of motion, and cervicogenic headache.3 Identifying the pattern and addressing contributing drivers can improve both short-term symptom relief and long-term postural resilience.
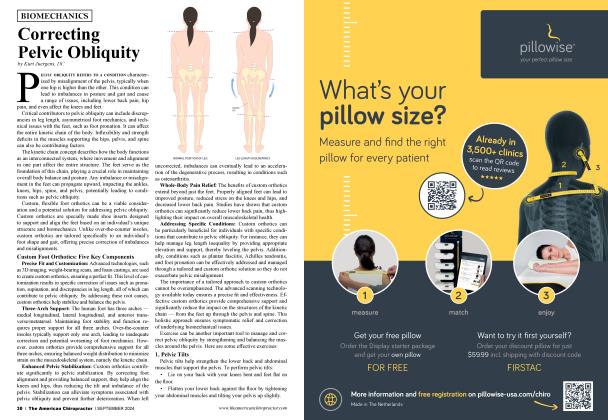
Cervical anterior translation refers to anterior displacement of the craniocervical complex relative to the thoracic cage. In a neutral standing posture, it is commonly observed when the external auditory meatus falls anterior to the acromioclavicular (AC) joint line.4
The pattern typically includes lower cervical flexion with compensatory upper cervical extension and may present with changes in the “bite line” and head-neck hinging.5 Classic clinical texts have long emphasized the mechanical cost of this position.
Cailliet19 20 noted that each inch of forward translation can substantially increase cervical muscular effort by approximately 10 pounds of tension. Curl20-21 described increased compressive loading in the lower cervical segments, particularly C5 to C7, due to a longer lever arm.
Common accompanying findings include rounded shoulders, increased thoracic kyphosis, humeral internal rotation, and soft-tissue thickening at the cervicothoracic junction.6 Recognizing FHP as a predictable cluster of compensations helps clinicians avoid treating the cervical spine in isolation and instead target the primary driver(s) of the pattern.
Forward head posture can also emerge as a compensation for distal dysfunction. For example, excessive foot pronation may shift the body’s center of mass anteriorly, prompting anterior pelvic translation to maintain balance.7 The thoracic spine may then adapt in an attempt to rebalance the upper body, with the cervical spine translating forward as part of the overall strategy.8-9
Christensen21-22 and Janda22-23 both emphasized that durable postural change is more likely when clinicians assess and address the full kinetic sequence, from the pedal foundation through the pelvis and thorax, while restoring joint stability and neuromuscular control. In practice, this may include manual care, targeted rehabilitation, and (when appropriate) supportive interventions to improve distal stability and reduce compensatory cervical load.
All of that makes the argument for custom orthotics to correct excess pronation, reestablish a proper center of gravity, and reduce compensatory changes in the kinetic chain.
From a neurological perspective, FHP can alter cervical afferent input and disrupt sensorimotor integration. Proprioceptive distortion has been associated with impaired balance, dizziness, and faulty postural control in some patients.8
Sustained anterior head posture often maintains tonic activity in the upper trapezius, levator scapulae, and suboccipital muscles, contributing to overuse fatigue and stiffness.9 This persistent neural drive may interfere with reflexive stability and head-eye coordination,10 and maladaptive sensory input from overloaded cervical receptors may contribute to cervicogenic headache and chronic pain patterns.13-14
Biomechanically, cervical anterior translation increases gravitational torque on the cervical spine. The cervical extensors must produce greater force to counterbalance the forward shift, which can accelerate fatigue and reduce postural endurance.15-16
At the same time, compressive loading on intervertebral discs and posterior elements increases, especially in the lower cervical segments.11 Over time, these forces may contribute to symptom persistence, particularly in individuals who maintain prolonged static postures.
FHP is also characterized by an imbalance between overactive superficial extensors and inhibited deep cervical flexors. This helps explain why manipulation alone may provide only temporary relief unless paired with neuromuscular reeducation and progressive loading strategies.18-19 A combined approach that addresses mobility, motor control, and endurance typically yields more durable improvements.
A rehabilitation plan should begin with a structured assessment; sagittal head-neck alignment, deep neck flexor endurance, scapular strength, and thoracic mobility are common clinical priorities.4,6
Evidence-informed intervention categories include:
• Cervical retraction control: gentle posterior translation drills to restore axial elongation and improve motor control.12
• Deep neck flexor strengthening: low-load isometrics targeting the longus colli and longus capitis to improve endurance and postural stabilization.23
• Scapular stabilization: strengthening the lower trapezius and serratus anterior to reduce rounded shoulders and secondary cervical load.13
• Thoracic mobility and extension training: thoracic mobilization and extension exercise to increase sagittal freedom and reduce compensatory cervical extension.14 Addressing excessive thoracic kyphosis may also be important for older adults because hyperkyphosis has been linked with increased fall risk.15,23
Dosage and progression should be individualized. Apractical framework is to progress from motor control to endurance and then to functional load-tolerance, aligning with modem exercise-therapy evidence supporting gradual adaptation.12-14
Nocturnal alignment can reinforce or undermine daytime postural correction. Pillow support that preserves a neutral cervical lordosis may reduce anterior shear and overnight strain.16
• Supine: a moderate cervical contour can support the natural curve while avoiding excessive extension.17
• Side-lying: pillow height should generally approximate the shoulder-to-neck distance to minimize lateral flexion.18
Inappropriate pillow height or a pillow that has degraded over time may encourage cervical flexion and perpetuate FHP; periodic reassessment is reasonable as fill materials compress.19
Cervical anterior translation increases tissue loading and alters neuromuscular coordination, making it a common contributor to ongoing neck pain and dysfunction. Because it often reflects broader kinetic-chain compensation, durable correction requires more than local cervical treatment. Integrating manual care with postural retraining, progressive stabilization, and appropriate sleep support offers the best path toward long-term resilience.
• Cervical anterior translation (FHP) is commonly identified when the ear lies anterior to the AC joint line, often accompanied by thoracic kyphosis and rounded shoulders.4-6
• Forward translation increases cervical muscular demand and compressive loading, particularly at C5 - C7.15-17
• Distal drivers, such as excessive pronation, may contribute to global compensations and should be assessed when indicated.7,14
• Altered cervical proprioception can affect sensorimotor control and may contribute to dizziness, headache, and persistent pain.8
• Durable improvement typically requires a combined strategy: manual care plus motor reeducation, mobility work, and endurance training.9-12
• Sleep posture and pillow support can reinforce corrective efforts when matched to the patient’s needs.16-18-19
Dr. Mark Charette is a 1980 summa cum laude graduate of Palmer College of Chiropractic and a former All-American swimmer. He is a frequent guest speaker at chiropractic colleges and has taught over 2,200 seminars worldwide on extremity adjusting, biomechanics, and spinal adjusting techniques. He has authored a book on extremity adjusting and produced an instructional video series. His lively seminars emphasize a practical, hands-on approach. As a Foot Levelers Speakers Bureau member, he travels the country sharing his knowledge and insights. Learn more at www.footlevelers.com/more.
1. Szeto GP, Straker LM, O'Sullivan PB. A comparison of symptomatic and asymptomatic office workers performing monotonous keyboard work — 1: neck and shoulder muscle recruitment patterns. Man Ther. 2005 Nov;10(4):270-80. doi: 10.1016/j.math.2005.01.004. Epub 2005 Jul 5. PMID: 15998595.
2. Page P, Frank CC, Lardner R. Assessment and treatment of muscle imbalance. Champaign, IL: Human Kinetics. 2010.
3. Kristjansson E, Treleaven J. Sensorimotor function and dizziness in neck pain: implications for assessment and management. J Orthop Sports Phys Ther. 2009 May;39(5):364-77. doi: 10.2519/ jospt.2009.2834. PMID: 19411769.
4. Kendall FP, McCreary EK, Provance PG. Muscles: testing and function. 5th ed. Baltimore: Williams & Wilkins. 2005.
5. Raine S, Twomey LT. Head and shoulder posture variations in 160 asymptomatic women and men. Arch Phys Med Rehabil. 1997 Nov;78(ll):1215-23. doi: 10.1016/s0003-9993(97)90335-x. PMID: 9365352.
6. Sahrmann S, Azevedo DC, Dillen LV. Diagnosis and treatment of movement system impairment syndromes. Braz J Phys Ther. 2017 Nov-Dec;21(6):391-399. doi: 10.1016/j.bjpt.2017.08.001. Epub 2017 Sep 27. PMID: 29097026; PMCID: PMC5693453.
7. Dananberg HJ. Gait style as an etiology to chronic postural pain. Part I: functional hallux limitus. Journal of the American Podiatric Medical Association. 1993;83*(8):433-441. doi: 10.7547/87507315-838-433
8. Treleaven J. Dizziness, Unsteadiness, visual disturbances, and sensorimotor control in traumatic neck pain. J Orthop Sports Phys Ther. 2017 Jul;47(7):492-502. doi: 10.2519/jospt.2017.7052. Epub 2017 Jun 16. PMID: 28622488.
9. Falia D, Bilenkij G, Juli G. Patients with chronic neck pain demonstrate altered patterns of muscle activation during performance of a functional upper limb task. Spine (Phila Pa 1976). 2004 Jul l;29(13):1436-40. doi: 10.1097/01.brs.0000128759.02487.bf PMID: 15223935.
10. Sterling M, Juli G, Wright A. Cervical facet joint pain: clinical signs, pathways, and management. Man Ther. 2001;6(2):72-81.
11. Cheng CH, Wong YW, Ju YH, et al. Deep cervical flexor training in chronic neck pain: a systematic review. Phys Ther. 2015;95(6):829-40.
12. Ludewig PM, Reynolds JF. The role of the scapula in shoulder impingement syndrome. JOrthop Sports Phys Ther. 2009;39(2):90-104.
13. Lau HM, Wing Chiu TT, Lam TH. The effectiveness of thoracic manipulation on patients with chronic mechanical neck pain — a randomized controlled trial. Man Ther. 2011 Apr;16(2): 141-7. doi: 10.1016/j.math.2010.08.003. Epub 2010 Sep 1. PMID: 20813577.
14. Kado DM, Huang MH, Karlamangla AS, et al. Thoracic hyperkyphosis and risk of falls among older community-dwelling women. J Gerontol A Biol Sci Med Sci. 2007;62(6):652-7.
15. Gordon SJ, Maul TL, Shields J, et al. Influence of cervicothoracic support during sleep on spinal loading. Ergonomics. 2005;48(2): 161-72.
16. Lavin RA, Perry P, Freehill A. Comparative evaluation of cervical pillow types on sleeping posture and pain. Clin Biomech. 2010;25(8):776-81.
17. Leilnahari K, Fard SA, Azamiraz SJ. Pillow height and shape influence on cervical alignment in side sleeping. J Manipulative Physiol Ther. 2011;34(2):107-13.
18. Erfanian P, Khosro A, Ghaffari M. Relationship between pillow shape and spinal alignment during sleep. J Biomech. 2017:60:21421.
19. Cailliet, R. Neck and arm pain (2nd ed.). F. A. Davis. 1981.
20. Curl DD. (Ed.). A chiropractic approach to head pain. Williams & Wilkins. 1994.
21. Christensen MG. The chiropractic story. Mosby-Year Book. 1991.
22. Janda V, Frank C, Liebenson C. (Eds.). Assessment and treatment of muscle imbalance: The Janda approach. Human Kinetics. 2008.
23. O'Leary S, Falla D, Elliott JM, Juli G. Muscle dysfunction in cervical spine pain: implications for assessment and management. J Orthop Sports Phys Ther. 2009 May;39(5):324-33. doi: 10.2519/ jospt.2009.2872. PMID: 19411767.