MEDICARE PATIENTS REPRESENT A Uniquely challenging and rewarding population within chiropractic practice. These individuals frequently present with chronic neuromusculoskeletal conditions, multiple co-morbidities and shaped by decades of cumulative spinal stress, degenerative change, and age-related physiological adaptation. Disc degeneration, spinal stenosis, osteoarthritis, postural collapse, and osteoporosis are no longer exceptions but commonplace.
Add in a multitude of pharmacological prescriptions, balance issues, and a risk for minor adverse events, such as their low threshold for post-treatment soreness, tissue fragility, and osteoporosis, and we have a growing patient population that requires special attention. These patients are the perfect candidates for an Instrument adjusting approach.
At the same time, the Medicare chiropractic benefit is narrow, highly regulated, and documentation driven. Coverage is limited to spinal manipulation for the active treatment of a spinal subluxation, and claims must clearly demonstrate medical necessity, functional impairment, and measurable response to care. Maintenance therapy is explicitly excluded (Centers for Medicare & Medicaid Services [CMS]).
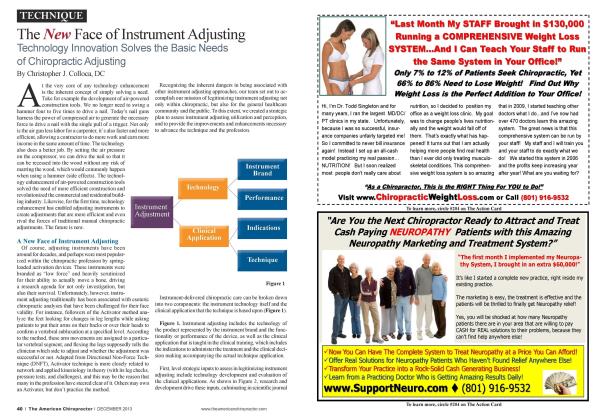
This dual reality places doctors of chiropractic (DCs) under increasing pressure to deliver care that is both clinically appropriate for vulnerable spinal tissues and defensible within Medicare’s documentation framework. Instrument-assisted adjusting, particularly modern electromechanical systems that provide targeted, specific, and controlled-force thrust delivery, offers a compelling solution for meeting both demands.
The Medicare Spine:
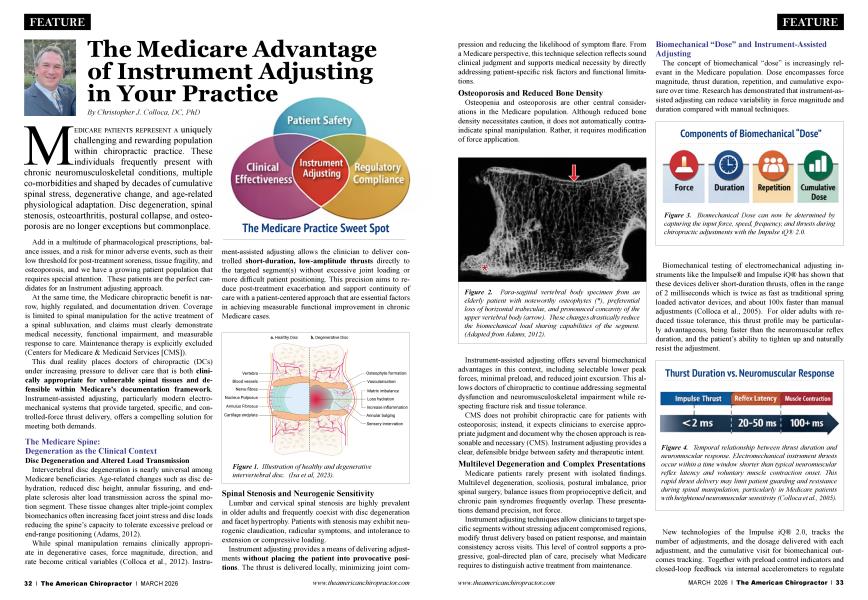
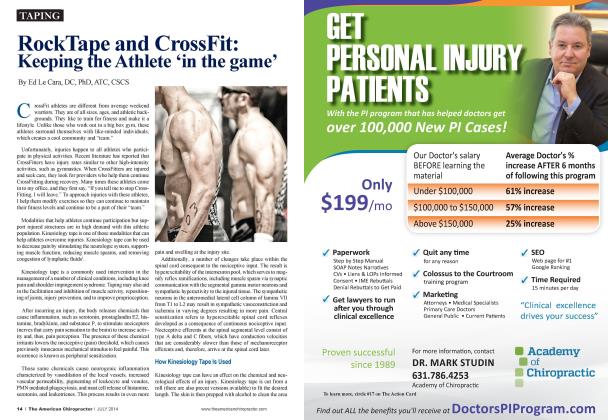
Intervertebral disc degeneration is nearly universal among Medicare beneficiaries. Age-related changes such as disc dehydration, reduced disc height, annular fissuring, and endplate sclerosis alter load transmission across the spinal motion segment. These tissue changes alter triple-joint complex biomechanics often increasing facet joint stress and disc loads reducing the spine’s capacity to tolerate excessive preload or end-range positioning (Adams, 2012).
While spinal manipulation remains clinically appropriate in degenerative cases, force magnitude, direction, and rate become critical variables (Colloca et al., 2012). Instrument-assisted adjusting allows the clinician to deliver controlled short-duration, low-amplitude thrusts directly to the targeted segment(s) without excessive joint loading or more difficult patient positioning. This precision aims to reduce post-treatment exacerbation and support continuity of care with a patient-centered approach that are essential factors in achieving measurable functional improvement in chronic Medicare cases.
 Figure 1. Illustration of healthy and degenerative intervertebral disc. (Isa et al, 2023).
Figure 1. Illustration of healthy and degenerative intervertebral disc. (Isa et al, 2023).
Lumbar and cervical spinal stenosis are highly prevalent in older adults and frequently coexist with disc degeneration and facet hypertrophy. Patients with stenosis may exhibit neurogenic claudication, radicular symptoms, and intolerance to extension or compressive loading.
Instrument adjusting provides a means of delivering adjustments without placing the patient into provocative positions. The thrust is delivered locally, minimizing joint compression and reducing the likelihood of symptom flare. From a Medicare perspective, this technique selection reflects sound clinical judgment and supports medical necessity by directly addressing patient-specific risk factors and functional limitations.
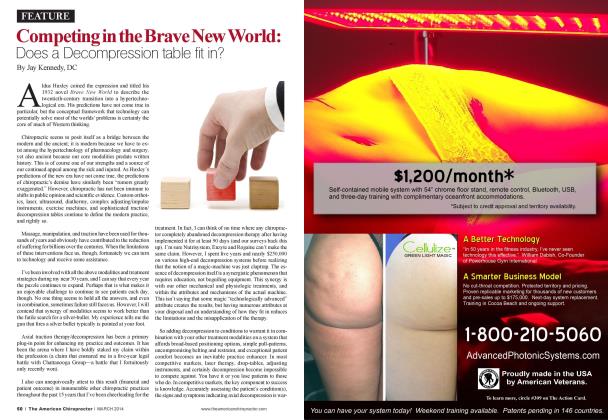
Osteopenia and osteoporosis are other central considerations in the Medicare population. Although reduced bone density necessitates caution, it does not automatically contraindicate spinal manipulation. Rather, it requires modification of force application.
 Figure 2. Para-sagittal vertebral body specimen from an elderly patient with noteworthy osteophytes (*), preferential loss of horizontal trabeculae, and pronounced concavity of the upper vertebral body (arrow). These changes drastically reduce the biomechanical load sharing capabilities of the segment. (Adapted from Adams, 2012).
Figure 2. Para-sagittal vertebral body specimen from an elderly patient with noteworthy osteophytes (*), preferential loss of horizontal trabeculae, and pronounced concavity of the upper vertebral body (arrow). These changes drastically reduce the biomechanical load sharing capabilities of the segment. (Adapted from Adams, 2012).
Instrument-assisted adjusting offers several biomechanical advantages in this context, including selectable lower peak forces, minimal preload, and reduced joint excursion. This allows doctors of chiropractic to continue addressing segmental dysfunction and neuromusculoskeletal impairment while respecting fracture risk and tissue tolerance.
CMS does not prohibit chiropractic care for patients with osteoporosis; instead, it expects clinicians to exercise appropriate judgment and document why the chosen approach is reasonable and necessary (CMS). Instrument adjusting provides a clear, defensible bridge between safety and therapeutic intent. Multilevel Degeneration and Complex Presentations
Medicare patients rarely present with isolated findings. Multilevel degeneration, scoliosis, postural imbalance, prior spinal surgery, balance issues from proprioceptive deficit, and chronic pain syndromes frequently overlap. These presentations demand precision, not force.
Instrument adjusting techniques allow clinicians to target specific segments without stressing adjacent compromisedregions, modify thrust delivery based on patient response, and maintain consistency across visits. This level of control supports a progressive, goal-directed plan of care, precisely what Medicare requires to distinguish active treatment from maintenance.
The concept of biomechanical “dose” is increasingly relevant in the Medicare population. Dose encompasses force magnitude, thrust duration, repetition, and cumulative exposure over time. Research has demonstrated that instrument-assisted adjusting can reduce variability in force magnitude and duration compared with manual techniques.
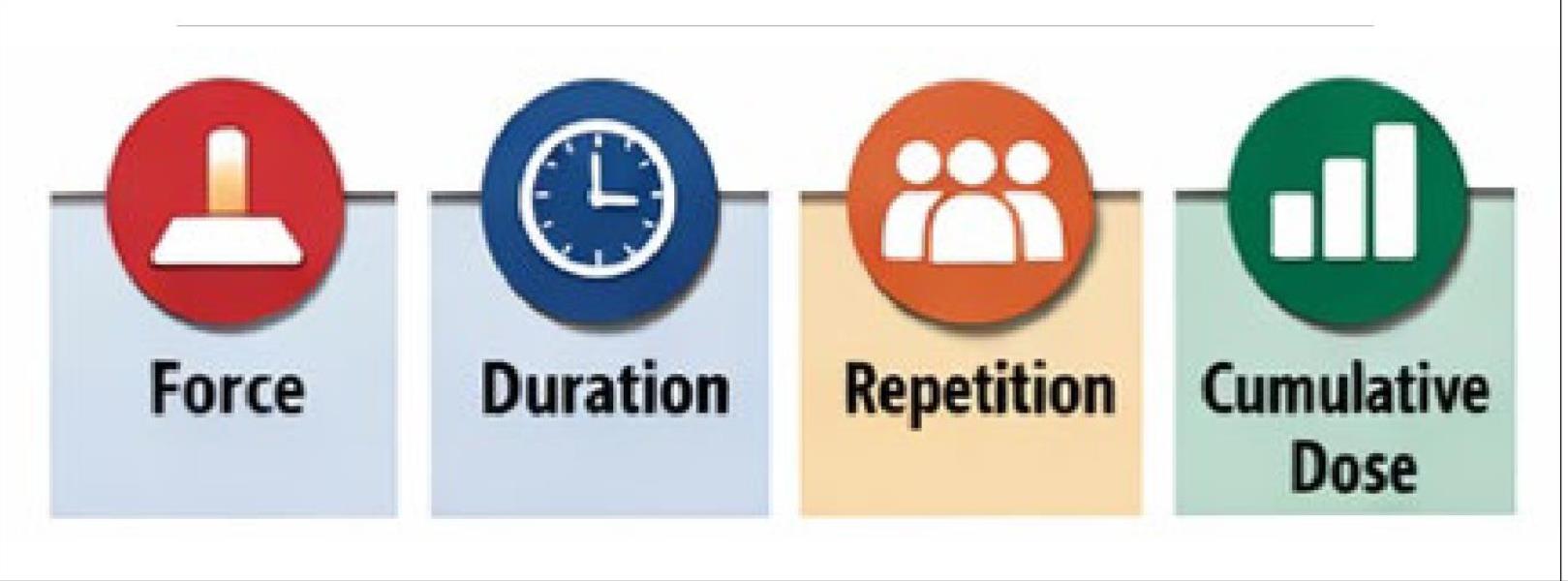 Figure 3. Biomechanical Dose can now be determined by capturing the input force, speed, frequency, and thrusts during chiropractic adjustments with the Impulse iQ® 2.0.
Figure 3. Biomechanical Dose can now be determined by capturing the input force, speed, frequency, and thrusts during chiropractic adjustments with the Impulse iQ® 2.0.
Biomechanical testing of electromechanical adjusting instruments like the Impulse® and Impulse iQ® has shown that these devices deliver short-duration thrusts, often in the range of 2 milliseconds which is twice as fast as traditional spring loaded activator devices, and about lOOx faster than manual adjustments (Colloca et al., 2005). For older adults with reduced tissue tolerance, this thrust profile may be particularly advantageous, being faster than the neuromuscular reflex duration, and the patient’s ability to tighten up and naturally resist the adjustment.
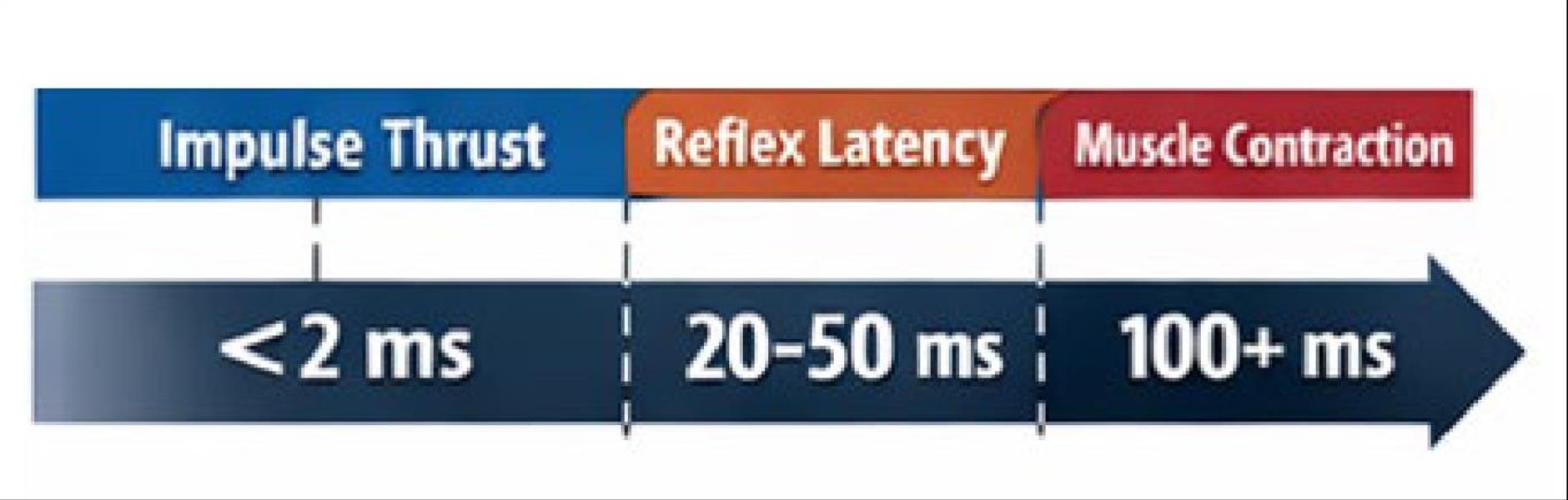 Figure 4. Temporal relationship between thrust duration and neuromuscular response. Electromechanical instrument thrusts occur within a time window shorter than typical neuromuscular reflex latency and voluntary muscle contraction onset. This rapid thrust delivery may limit patient guarding and resistance during spinal manipulation, particularly in Medicare patients with heightened neuromuscular sensitivity (Colloca et al., 2005).
Figure 4. Temporal relationship between thrust duration and neuromuscular response. Electromechanical instrument thrusts occur within a time window shorter than typical neuromuscular reflex latency and voluntary muscle contraction onset. This rapid thrust delivery may limit patient guarding and resistance during spinal manipulation, particularly in Medicare patients with heightened neuromuscular sensitivity (Colloca et al., 2005).
New technologies of the Impulse iQ® 2.0, tracks the number of adjustments, and the dosage delivered with each adjustment, and the cumulative visit for biomechanical outcomes tracking. Together with preload control indicators and closed-loop feedback via internal accelerometers to regulate thrust delivery, adjustments are controlled using patented patient-centered technology. Advancing this concept further, clinicians can now measure and monitor thrust delivery, allowing internal assessment of adjustment dosage across visits.
While Medicare does not require documentation of thrust force values, the ability to track dosage supports:
• Consistency in thrust delivery.
• Intentional modification based on patient tolerance and response.
• Clinical decision-making that reflects active management rather than repetitive care.
 Figure 5. Impulse iQ® 2.0 (Neuromechanical Innovations, Phoenix, AZ, USA) is equipped with an LCD display to capture chiropractic adjustment parameters including dosage.
Figure 5. Impulse iQ® 2.0 (Neuromechanical Innovations, Phoenix, AZ, USA) is equipped with an LCD display to capture chiropractic adjustment parameters including dosage.
For patients with spinal challenges such as disc degeneration, spinal stenosis, or osteoporosis, this measured approach allows clinicians to scale care appropriately while progressing, regressing, or maintaining thrust parameters as objective findings evolve.
Medicare Required Documentation
Medicare’s coverage for chiropractic services are limited to manual manipulation to correct a spinal subluxation, billed under CPT codes 98940-98942 (CMS). You are required to document medical necessity, functional change, and active treatment parameters with the rigor Medicare expects.
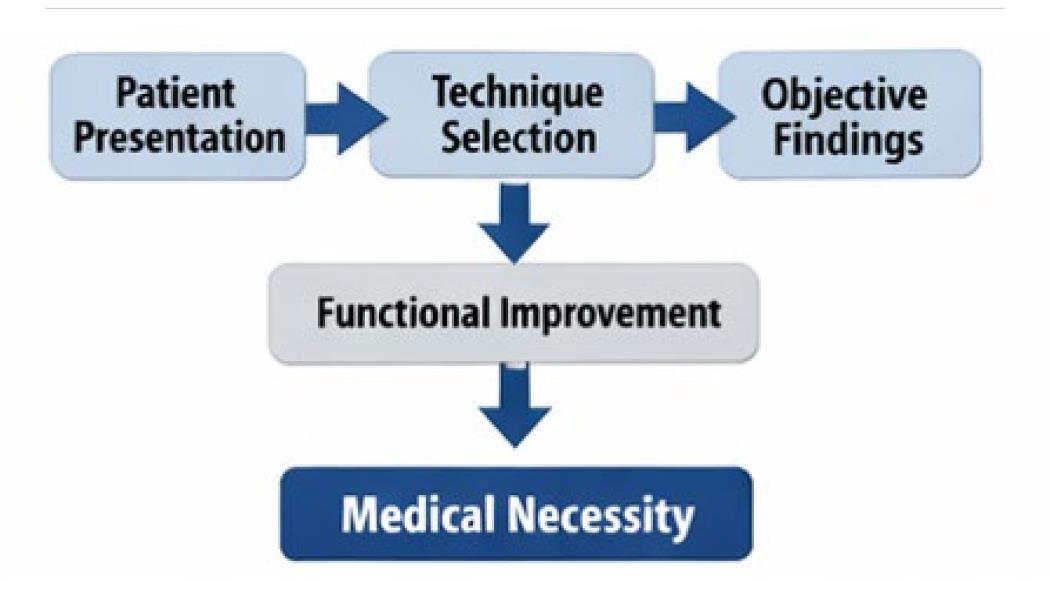 Figure 6. Technique selection based upon patient presentation in the Medicare population is a great example of patient-centered care.
Figure 6. Technique selection based upon patient presentation in the Medicare population is a great example of patient-centered care.
n Alignment
To establish medical necessity, documentation must demonstrate:
• A spinal subluxation identified by physical examination or imaging.
• A neuromusculoskeletal condition related to the subluxation.
• Functional impairment meaningful to daily activities.
• A reasonable expectation of improvement or arrest of progression.
CMS recognizes the commonly used PART framework— Pain/tenderness, Asymmetry/misalignment, Range of motion abnormality, and Tissue tone changes—when subluxation is identified via physical examination (CMS). Ongoing documentation must show that care remains active and corrective, not maintenance. The AT modifier may be used to indicate active treatment but does not, by itself, establish medical necessity (CMS).
As defined by Medicare, chiropractors may use manual devices (that is, those that are hand-held with the thrust of the force of the device being controlled manually) in performing manual manipulation of the spine. CMS is explicit that Medicare covers chiropractic care only when it is active/corrective treatment of a spinal subluxation and not maintenance care, and that documentation must demonstrate that distinction.
Chiropractic adjusting instruments are regulated by the US Food and Drug Administration under strict adherence to manufacturer’s safety and compliance with ISO 13485 medical device specifications and a Quality Management System. Beware of instruments that are made in China and not FDA cleared or registered, or those repaired or serviced by unregistered individuals that have opened repair shops in their garage. In a medicolegal situation, this will be the first evidentiary claim against you, and if you are found using a rogue device, not only will you put your case at enormous risk, further, you may not be covered by your malpractice carrier for blatant non-compliance of FDA statues.
Instrument adjusting fits well within Medicare’s documentation framework when records clearly link technique selection to patient presentation. Documentation should emphasize:
• Why a targeted, controlled-force approach is appropriate given degenerative findings.
• What objective changes are occurring over time.
• How functional capacity is improving or being preserved.
In chronic degenerative cases, improvement may be incremental. CMS acknowledges that chronic conditions can remain active when documentation demonstrates ongoing functional gains or prevention of deterioration (CMS).
When instrument adjusting is selected due to patient tolerance, osteoporosis risk, or neurogenic sensitivity, that reasoning strengthens the medical necessity narrative rather than weakening it.
Why Instrument Adjusting Is a Strategic Fit for the Medicare Practice
For Medicare beneficiaries, instrument-assisted adjusting provides:
• Targeted segmental specificity.
• Controlled-force delivery appropriate for degenerative spines.
• Reduced positional and compressive stress
• Improved tolerance and adherence to care.
For chiropractic practices, it supports:
• Consistency across providers and visits.
• Clear clinical reasoning tied to documentation.
• Aligmnent with Medicare’s active care requirements.
Medicare patients deserve chiropractic care that respects the realities of the aging spine while remaining firmly grounded in clinical effectiveness and regulatory compliance. Instrument-assisted adjusting when applied thoughtfully and documented rigorously meets this standard with outcomes-based patient-centered care.
By offering a targeted, specific, and controlled-force approach, instrument adjusting techniques are uniquely suited to managing disc degeneration, spinal stenosis, osteoporosis, and other complex spinal conditions common in the Medicare population. For doctors of chiropractic committed to precision care and sustainable practice growth, instrument adjusting represents not merely a technique choice, but a clinically sound evolution of care.

Chris Colloca, DC, PhD, is the CEO and Founder of Neuromechanical Innovations, manufacturer of the Impulse family of adjusting instruments in use in over 20,000 clinics worldwide in over 50 countries delivering nearly 1 Billion adjustments annually. More information can be found at www.Neuromechanical.com.
1. Adams MA. Basic science of spinal degeneration. (2012). Surgery ^Oxford) 30(7), 347-350.
2. Centers for Medicare & Medicaid Services. Chiropractic services, https://www.cms.gov
3. Centers for Medicare & Medicaid Services. Medicare benefit policy manual (Pub. 100-02), Chapter 15: Covered medical and other health services.
4. Colloca, C. J., Keller, T. S., Black, P, Normand, M. C., Harrison, D. E., & Harrison, D. D. (2005). Comparison of mechanical force of manually assisted chiropractic adjusting instmments. J Manipulative Physiol Ther, 28(6), 414-422.
5. Colloca CJ, Gunzburg R, Freeman BJ, Szpalski M, Afifi M, Moore RJ. (2012). Biomechanical quantification of pathologic manipulable spinal lesions: an in vivo ovine model of spondylolysis and intervertebral disc degeneration. J Manipulative Physiol Ther, 35(5), 354-66.
6. Isa ILM, Teoh SL, Nor NHM, Mokhtar SA. (2023). Discogenic low back pain: anatomy, pathophysiology and treatments of intervertebral disc degeneration. Int J Mol Set, 24(1), 208-24.