PINPOINTING THE ETIOLOGY OF A CHRONIC cough can be difficult, but after numerous standard-of-care tests, the diagnosis was that my “non-pathogenic” cough was the result of nerve irritation around the larynx caused by an anesthesia tube insert that seemed to reset my coughing reflex.
Until this happened, I was unaware of how common this condition is and how often it goes undiagnosed. I was sent to a speech therapist who basically recommended things that stimulate the vagus nerve, and I was told to swallow water slowly because you can’t swallow and cough at the same time. That was 2015, and I continued with the annoying albeit nonpathological cough for the next decade.
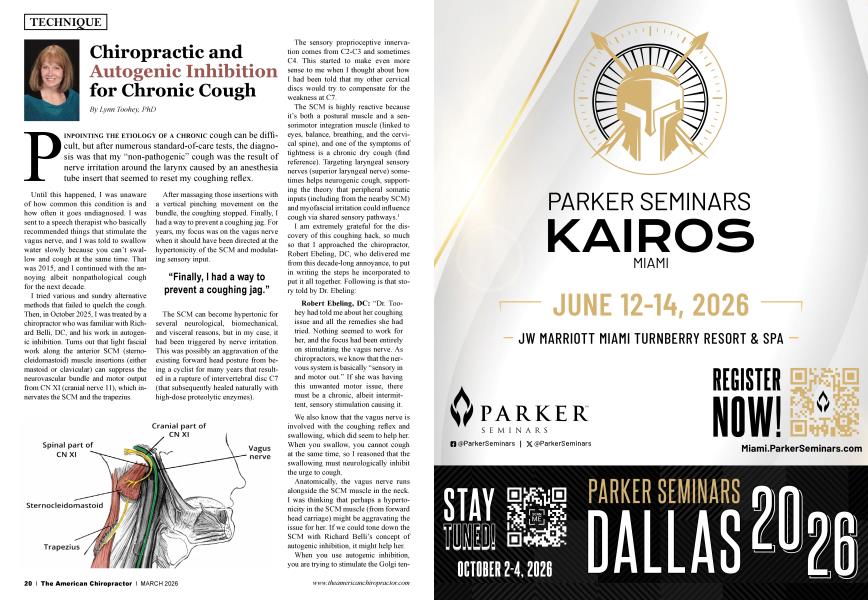
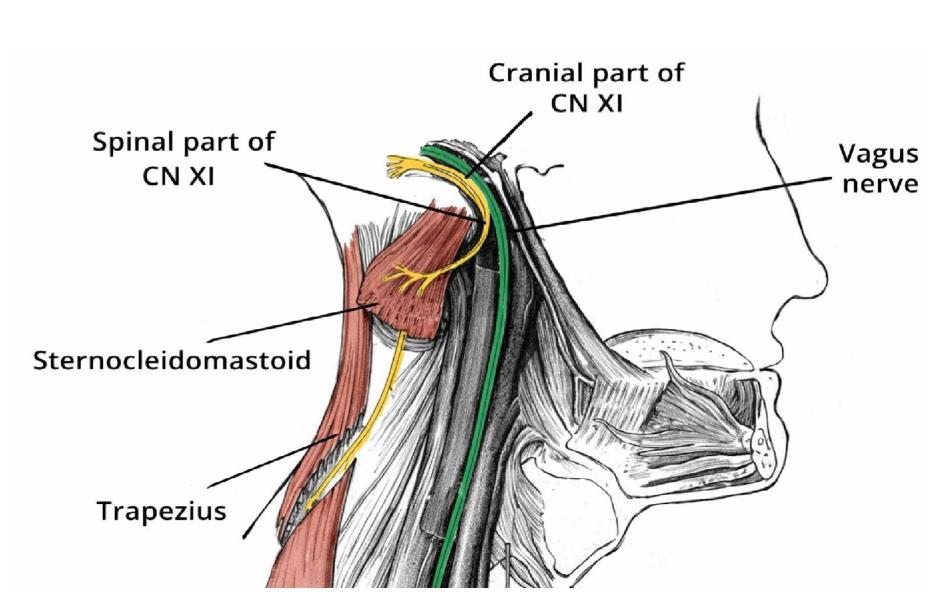
I tried various and sundry alternative methods that failed to quelch the cough. Then, in October 2025,1 was treated by a chiropractor who was familiar with Richard Belli, DC, and his work in autogenic inhibition. Turns out that light fascial work along the anterior SCM (sternocleidomastoid) muscle insertions (either mastoid or clavicular) can suppress the neurovascular bundle and motor output from CN XI (cranial nerve 11), which innervates the SCM and the trapezius.
After massaging those insertions with a vertical pinching movement on the bundle, the coughing stopped. Finally, I had a way to prevent a coughing jag. For years, my focus was on the vagus nerve when it should have been directed at the hypertonicity of the SCM and modulating sensory input.
“Finally, I had a way to prevent a coughing jag.”
The SCM can become hypertonic for several neurological, biomechanical, and visceral reasons, but in my case, it had been triggered by nerve irritation. This was possibly an aggravation of the existing forward head posture from being a cyclist for many years that resulted in a rupture of intervertebral disc C7 (that subsequently healed naturally with high-dose proteolytic enzymes).
The sensory proprioceptive innervation comes from C2-C3 and sometimes C4. This started to make even more sense to me when I thought about how I had been told that my other cervical discs would try to compensate for the weakness at C7.
The SCM is highly reactive because it’s both a postural muscle and a sensorimotor integration muscle (linked to eyes, balance, breathing, and the cervical spine), and one of the symptoms of tightness is a chronic dry cough (find reference). Targeting laryngeal sensory nerves (superior laryngeal nerve) sometimes helps neurogenic cough, supporting the theory that peripheral somatic inputs (including from the nearby SCM) and myofascial irritation could influence cough via shared sensory pathways.1
I am extremely grateful for the discovery of this coughing hack, so much so that I approached the chiropractor, Robert Ebeling, DC, who delivered me from this decade-long annoyance, to put in writing the steps he incorporated to put it all together. Following is that story told by Dr. Ebeling:
Robert Ebeling, DC: “Dr. Toohey had told me about her coughing issue and all the remedies she had tried. Nothing seemed to work for her, and the focus had been entirely on stimulating the vagus nerve. As chiropractors, we know that the nervous system is basically “sensory in and motor out.” If she was having this unwanted motor issue, there must be a chronic, albeit intermittent, sensory stimulation causing it.
We also know that the vagus nerve is involved with the coughing reflex and swallowing, which did seem to help her. When you swallow, you cannot cough at the same time, so I reasoned that the swallowing must neurologically inhibit the urge to cough.
Anatomically, the vagus nerve runs alongside the SCM muscle in the neck. I was thinking that perhaps a hypertonicity in the SCM muscle (from forward head carriage) might be aggravating the issue for her. If we could tone down the SCM with Richard Belli’s concept of autogenic inhibition, it might help her.
When you use autogenic inhibition, you are trying to stimulate the Golgi tendon organ (GTO) located in the tendons of the muscle. The GTO, when it detects a contraction, reversely inhibits a muscle from firing more to prevent injury.
The technique is quite easy to perform. You get down around the tendon area of the SCM, where it attaches to the clavicle, and you pinch the muscle in a vertical direction, trying to approximate the muscle fibers to make the GTO think a muscle contraction is happening.
There are also GTOs at the other end of the SCM, where it attaches to the mastoid process. I told her to play around with different locations and see what worked best. She reported that using the technique, moving from the belly of the muscle to the GTO attachment near the trapezius, seemed to work best.
In hypothesizing why this works, it could be that, since palpation of the SCM indirectly affects vagal tone and is one of the techniques used to “reset” vagal tone, it’s possible that this method tones down the SCM and sends sensory information to the vagus nerve, decreasing motor output. We know that the vagus nerve runs deep to the SCM and that working the SCM can indirectly modulate vagal tone by way of its effects on the carotid sheath and/or baroreceptors.
We also know that hypertonicity of the SCM can mimic vagus-related symptoms, such as dizziness and nausea, not because of vagus innervation but because of vestibular and proprioceptive crossover. Cervical region tightness has been discovered to cause vagal-related problems, and soft tissue relaxation of the cervical region has been found to relieve gastric symptoms.2
Whatever the answer is, it does seem to help her. Experiment with the techniques on your patients, keeping in mind that you want to initiate autogenic inhibition in the right area and with the correct movement, as simple pressure on the SCM has also been known to trigger the cough reflex.”3
Richard Belli, DC: “Autogenic inhibition can be executed in two ways. First of all, autogenic inhibition can be used on the tendons by compressing or pinching the actual tendon itself with light pressure. The tendons actually don’t have stretch receptors but are pressure receptors. Therefore, pinching the tendons makes the brain think that the muscle is being overstretched, thus the inhibitory signal to the alpha motor neuron.
The second version is by approximating and pinching the muscle spindle in the belly of the muscle, which also results in an inhibitory signal to the alpha motor neuron. It was interesting that the positive outcome sounds as if both versions were applied, since the pinching motion was initiated with the knuckle of the index finger placed on the belly of the muscle spindle, combined with the thumb placed on the tendon near the trapezius.”
Knowing that certain nutrients, such as magnesium and taurine, would help with the muscle relaxation, I started taking a supplement with both ingredients in the formula. I wanted a magnesium that would be efficient and absorbable, so I used a combination formula that combined malate, citrate, and glycinate as chelators for magnesium.
Malate, citrate, and glycinate are exceptional carriers for magnesium that greatly increase the absorption rate of magnesium into the system. Utilizing all three of these carriers takes advantage of the nutritional benefits of each one. Choosing these forms over other, less absorbable forms can make a big difference in overall magnesium absorption.
The science is there to support the fact that magnesium is known as a muscle relaxant and vasodilator.4 A systematic review noted decreased muscle soreness, improved performance, and a protective effect on muscle damage with magnesium supplementation, boosting the evidence that magnesium has a strong effect on muscle.5
Items that deplete or interfere with magnesium absorption include alcohol, soda, tea (not herbal), coffee, chocolate, sugar, herbicides, antibiotics, diuretics, and medications that affect kidney function. Impaired digestion, aging, disease, stress, intense exercise, surgery, diarrhea, vomiting, and illness (especially affecting the digestive/intestinal area) can also reduce magnesium absorption.
Taurine can also be important for muscle relaxation. Taurine is abundant in skeletal muscle and helps with calcium homeostasis and membrane stabilization, both of which are critical for proper muscle contraction/relaxation cycles.6 Supplementation with taurine has also been shown to improve muscle mitochondrial and respiratory metabolism, which also supports muscle health, endurance, and efficient contraction/relaxation.
In summary, the etiology of a neurogenic cough can vary, but it can be useful to experiment with and incorporate efficacious protocols that can work to help calm hypertonic muscles that are aggravating sensory input. Utilizing autogenic inhibition and nutrition as an accessory application can further support the goal of reducing muscle tightness and inhibiting overactive muscles.

Dr. Lynn Toohey organizes seminars, acts as a nutritional consultant to Nutri-West (www.NutriWest.com) and authored the Functional Health Evaluation program that analyzes blood tests and DNA raw data (www.FHEcloud.com). Dr. Toohey can be reached at [email protected] with any questions.
1. Dhillon VK. Superior laryngeal nerve block for neurogenic cough: a case series. Laryngoscope Investig Otolaryngol. 2019 Jul 5;4(4):410-413. doi: 10.1002/lio2.292. PMID: 31453350; PMCID: PMC6703134.
2. Ozel Asliyuce Y, Berberoglu U, Ulger O. Is cervical region tightness related to vagal function and stomach symptoms? Med Hypotheses. 2020 Sep;142:109819. doi: 10.1016/j.mehy.2020.109819. Epub 2020 May 6. PMID: 32408072.
3. Mannini C, Bemacchi G, Bond V, Cinelli E, Mutolo D, Fontana GA, Lavorini F. Somatic points for cough and urge to cough in chronic coughers. Respir Med. 2022 Aug-Sep;200:106929. doi: 10.1016/j. rmed.2022.106929. Epub 2022 Jul 14. PMID: 35853267.
4. Liguori S, Moretti A, Paoletta M, Gimigliano F, lolascon G. Role of magnesium in skeletal muscle health and neuromuscular diseases: a scoping review. Int J Mol Set. 2024 Oct 18;25(20): 11220. doi: 10.3390/ ijms252011220. PMID: 39457008; PMCID: PMC 11508242.
5. Tarsitano MG, Quinzi F, Folino K, Greco F, Oranges FP, Cerulli C, Emerenziani GP. Effects of magnesium supplementation on muscle soreness in different type of physical activities: a systematic review. J Transl Med. 2024 Jul 5;22(1):629. doi: 10.1186/sl2967024-05434-x. PMID: 38970118; PMCID: PMC 11227245.
6. De Luca A, Piemo S, Camerino DC. Taurine: the appeal of a safe amino acid for skeletal muscle disorders. J Transl Med. 2015 Jul 25;13:243. doi: 10.1186/sl2967-015-0610-l. PMID: 26208967; PMCID: PMC4513970.
7. Netter, Frank MD. The CIBA collection of medical illustrations. Vol 1. Nervous System and Part 1. Anatomy and Physiology. 1983. CIBA Pharmaceutical Co.