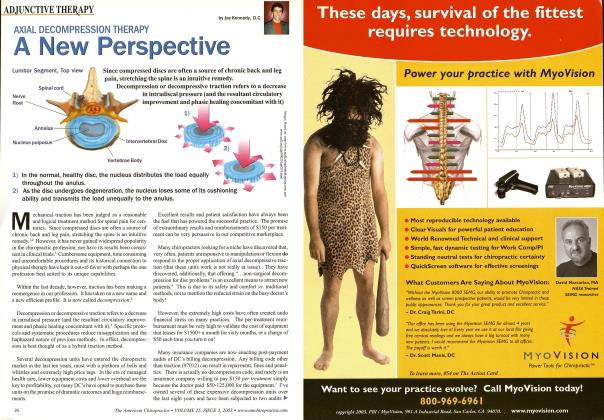
Movement, Modality, or Both: Decompression Technique Insights
TECHNIQUE
By Jay Kennedy, DC
Most would agree that a big key to patient care is efficient and accurate patient classification. During the past decade, the terms “patient classification,” “subgrouping,” and “clinical prediction rules” have become ubiquitous in physical medicine research.1 Chiropractic techniques all have their own set of criteria to decide who is or isn’t a candidate for the treatment. Since most chiropractic treatments involve motion, gradual motion, assisted motion, or intense motion, it’s important to recognize when motion isn’t the preferable treatment mode, or when consideration should be given to achieving simultaneous effects. Modalities were developed as an option of treatment for those in acute, traumatically induced tissue injury (motion avoidance), and to supplement those in subacute and chronic pain conditions. Modalities such as ultrasound also can improve exercise benefits.2
When we first encounter a patient in acute, intractable, or unendurable pain, many of us may honestly think, “What do you think I can do for you?” We then remember our oath (and our office expenses) and try to get to work. Fortunately, there are innumerable methods and devices available to help us address the acute presentations). Most of these methods tend to be under the banner of electric modalities. Creams, tapes, heat, and ice all serve a viable purpose, although most can be self-administered, but electric devices have a long history of successfully gating and subduing pain and generating a sense of direction for the acute-pained patient. A problem with the term “acute” is not so much the duration of the pain (typically anywhere from a week to a month), but the intensity and tissue source. An acute HNP may be well suited for decompression or manipulation from the initial encounter, but a rotational sprain of the disc’s outer wall may never be well suited for the treatment. The same holds true for facet involvement and muscle strains. Systematic reviews are less than encouraging than definitive findings to prove the source of back pain, but a comprehensive assessment involving facilitated motions, centralization response, disfraction tolerance, morning pain, etc. can all help narrow the culprit and better define the treatment choice.3 It’s also worth noting that even though we tend to blame “instability issues” for chronic pain, it’s pretty clear
that most pain is postural and likely from degenerate discs that have lost load-transfer capacities.4 5
I have been involved with laser therapy for more than a decade, and like many, I have fried most every unit available. However, I quickly morphed from the “cold” Class III lasers to the “hot” Class IV lasers when they became available and made them an intricate part of our protocols. I have a tendency to group laser clinicians into two categories: those who have recognized the efficacy and potency of Class IV Lasers, and those who have never used one (and therefore don’t know what they’re actually missing). Of course, there is the additional category of those with a financial stake in perpetuating the untenable proposition that a laser, which allows actual heat and numerous benefits, is somehow “damaging” to the body and will result in tissue injury. This is absurd in all regards, but dangerous for doctors who believe it and avoid their use. When doctors ask us about Class IV laser therapy vs. cold lasers for typical conditions we are treating (neck, back, and disc conditions), my response is typically:
1. If the patient can’t feel it, I doubt it’s doing much good, and perhaps most importantly,
2. If the patient can’t feel it, they ai e less likely to want to pay for it.
It seems a very simple and realistic premise. When I began using my first Class IV laser, I was blown away not only by the pain relief and restoration of motion that occurred in most cases, but also by the patient’s understanding of its value from the very
first moment of application (something that was missing with cold lasers). Scientific theories about photobiologic, photochemical chromophores, etc. are interesting, but feeling direct and substantial deep heat is irreplaceable from a marketing vantage point. The fact that lasers must be a cash service opens up both substantial reimbursement potential and
a substantial stumbling block if the “wow factor” is absent. Additionally, of course, aie the innumerable “light” therapy devices available to the public on the Internet. When we used “cold lasers,” I would often be asked, “Are you actually doing something or just trying to scam me?” That question more than any other piqued my initial interest in “hot” lasers.
In our patient classification assessments, we aie generally creating three categories: compression (typically disc/nerve), movement disorder (inappropriate muscle activation patterns/ fixations/pelvic asymmetries and rotations), and sprain/strain (perhaps an acute annular tear or other innervated peripheral tissues). Obviously, the latter are generally motion-tolerant conditions, while the former are less so, at least in some points of care. The further considerations aie whether a combination of treatments is warranted. I began developing an “open” modality belt several years ago in an effort to improve patient tolerance to traction therapy, enhance treatment effects, and speed up office flow by doing two things at once—laser and decompression. In addition, the “open belt” afforded the clinician a direct, hands-on, vertebra-specific decompression procedure if needed. This effectively combines a hands-on methodology with decompression therapy. Patient response was excellent and it has become a very popular product worldwide. The premise of this synergy decompression is to enhance the effects by compounding the therapies. It appears that when properly classified as a prone-responsive condition, adding Class IV laser to decompression, hands-on protocols, and drop adjusting creates an enhancement of outcome. The proper patient classification obviously improves outcomes, but perhaps more importantly, it reduces iatrogenic issues and loss of patient confidence. When we recognize a disc compression attribute along with a moderate acute or subacute presentation, the application of laser simultaneously can play an important role. It also can reduce post-traction reactions by pain gating, as well as the analgesia of direct deep heat. 5 When pelvic asymmetry/ rotation is recognized, the judicious use of a drop-adjustment technique can be very helpful.6
When we recognize that some patient conditions must be nursed with modalities and the avoidance of motion, it makes sense to have them available. It’s also important to transfer that clinical decision to the patient; many patients appreciate a nonaggressive approach in the early stages and don’t need convincing. We too often hear of decompression practices impatiently wanting to get everyone in acute “disc” pain (or apparently
^ ^1 began developing an “open” modality belt several years ago in an effort to improve patient tolerance to traction therapy, enhance treatment effects, and speed up office flow by doing two things at once— laser and decompression. 5 5
so) onto the table. There is a mistaken assumption that since traction is less aggressive than a thrust, then somehow it doesn’t qualify as a movement therapy. This can occasionally irritate some spinal and extra-spinal structures when misapplied. Also, the imbibition of fluid adds an additional stress that can incite an annular compromise, generating a fair degree of pain and disability. We always assess for extension/flexion and distraction tolerance, and rarely choose decompression when not apparent. No matter the potency of a modality, it can never abrogate the distress created by inappropriate movement. In cases when a clear indication is not apparent, we suggest a short and very minimal decompression session with laser, getting the patient off the table within five or six minutes (four or five 30-second pulls). Low dose decompression will give us good prognostic insight, but avoid any really serious reactions.7 We use the expression “sweeping compression out of the way” at least temporarily with traction. This gives us better insight into distraction tolerance, imbibition tolerance, and the underlying impact of disordered-movement-patterns. After decompression reduces compression, it’s interesting how effective form-closure procedures can become. It’s also important to recognize how inflammation intersects with pain. With the potency of Class IV laser, we often see a robust improvement in range of motion as well as pressure-pain thresholds, giving us additional prognostic insight as to the extent of local inflammation. Over pressure or over thrust on locally inflamed regions can be counterproductive, as can traction that is too aggressive.
1. Johnson C, JMPT editorial. 2010
2. The effects of continuous ultrasound on cNSLBP. Ebedi S, et al. BMC Musculo Oct. 2012.
3. Effects of backward bending on lumbar IVD. Adams MA, et al Spine Feb 2000.
4. Delayed trunk muscle reflex responses increase risk of LB injury. Cholewicki J, et al Spine Dec 2005.
5. IVD disc mechanics as revealed by stress profilometry. McNally DS, et al, Spine 17 Jan 1992.
6. Shamberger W. Pelvic malalignment syndrome. Churchill Livingstone 2002
7. Grieves. Modern manual therapy. Lippincott 1986.
Kennedy is a 1987 graduate of Palmer Chiropractic College and maintains a full time practice in western Pennsylvania. He is the principal developer of the Kennedy Decompression Technique. Dr Kennedy teaches his nonmachine specific technique to practitioners who want to learn clinical expertise required to apply this increasingly mainstream therapy.
Kennedy Decompression Technique Seminars are approved for CE through various Chiropractic Colleges. The author can be contacted (a, drdecompression dfiennedytechnique, com