Hamstring (HS) injuries are the most common soft tissue injuries seen in team field sports and track. The pain in a hamstring syndrome typically radiates down the posterior thigh or popliteal region and is exacerbated by any activity that stretches the hamstrings.
Symptoms that can be related to an acute or chronic unresolved hamstring injury include sacroiliac joint pain/ strain, hip bursitis, tibial stress fracture and shin splints, hip impingement syndrome, pelvic pain (i.e., posterior ilium on the left, anterior/medial ilium on the right), pubalgia, recurrent hamstring pull (after a first or second occurrence), anterior knee pain, and posterior hip capsule gets very stiff. Make sure to include a posterior capsule stretch in the corrective program if that is the case. Eighty percent of hamstring injuries involve the long head of the biceps femoris. The biceps femoris muscle-tendon junction extends the full length of its muscle belly. Bicep femoris injuries without tendon disruption have a recovery time of about 21 days; those with tendon disruption treated nonoperatively recover in about 72 days.
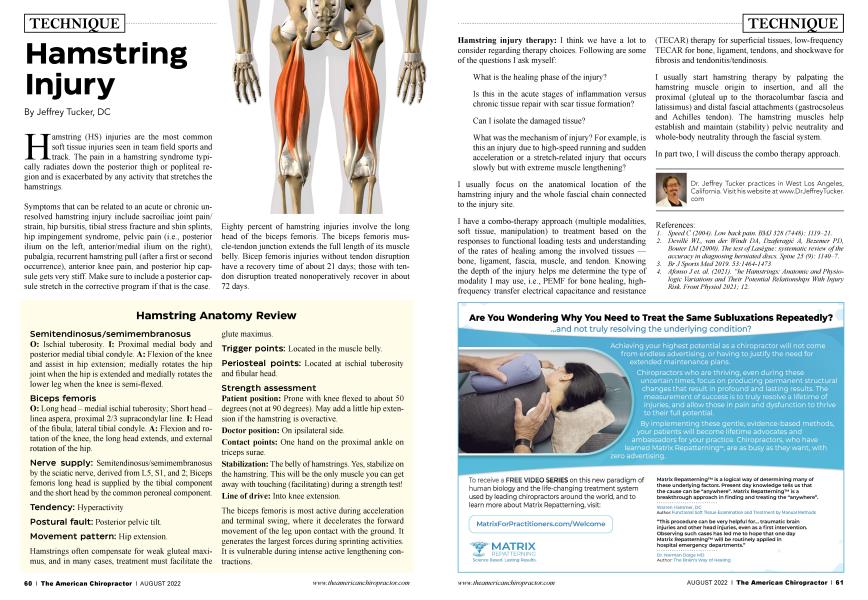
Hamstring Anatomy Review
Semitendinosus/semimembranosus
O: Ischial tuberosity. I: Proximal medial body and posterior medial tibial condyle. A: Flexion of the knee and assist in hip extension; medially rotates the hip joint when the hip is extended and medially rotates the lower leg when the knee is semi-flexed.
Biceps femoris
O: Long head - medial ischial tuberosity; Short head -linea aspera, proximal 2/3 supracondylar line. I: Head of the fibula; lateral tibial condyle. A: Flexion and rotation of the knee, the long head extends, and external rotation of the hip.
Nerve supply: Semitendinosus/semimembranosus by the sciatic nerve, derived from L5, SI, and 2; Biceps femoris long head is supplied by the tibial component and the short head by the common peroneal component.
Tendency: Hyperactivity
Postural fault: Posterior pelvic tilt.
Movement pattern: Hip extension.
Hamstrings often compensate for weak gluteal maximus, and in many cases, treatment must facilitate the
glute maximus.
Trigger points: Located in the muscle belly.
Periosteal points: Located at ischial tuberosity and fibular head.
Strength assessment
Patient position: Prone with knee flexed to about 50 degrees (not at 90 degrees). May add a little hip extension if the hamstring is overactive.
Doctor position: On ipsilateral side.
Contact points: One hand on the proximal ankle on triceps surae.
Stabilization: The belly of hamstrings. Yes, stabilize on the hamstring. This will be the only muscle you can get away with touching (facilitating) during a strength test! Line of drive: Into knee extension.
The biceps femoris is most active during acceleration and terminal swing, where it decelerates the forward movement of the leg upon contact with the ground. It generates the largest forces during sprinting activities. It is vulnerable during intense active lengthening contractions.
Hamstring injury therapy: I think we have a lot to consider regarding therapy choices. Following are some of the questions I ask myself:
What is the healing phase of the injury?
Is this in the acute stages of inflammation versus chronic tissue repair with scar tissue formation?
Can I isolate the damaged tissue?
What was the mechanism of injury? For example, is this an injury due to high-speed running and sudden acceleration or a stretch-related injury that occurs slowly but with extreme muscle lengthening?
I usually focus on the anatomical location of the hamstring injury and the whole fascial chain connected to the injury site.
I have a combo-therapy approach (multiple modalities, soft tissue, manipulation) to treatment based on the responses to functional loading tests and understanding of the rates of healing among the involved tissues — bone, ligament, fascia, muscle, and tendon. Knowing the depth of the injury helps me determine the type of modality I may use, i.e., PEMF for bone healing, highfrequency transfer electrical capacitance and resistance (TECAR) therapy for superficial tissues, low-frequency TECAR for bone, ligament, tendons, and shockwave for fibrosis and tendonitis/tendinosis.
I usually start hamstring therapy by palpating the hamstring muscle origin to insertion, and all the proximal (gluteal up to the thoracolumbar fascia and latissimus) and distal fascial attachments (gastrocsoleus and Achilles tendon). The hamstring muscles help establish and maintain (stability) pelvic neutrality and whole-body neutrality through the fascial system.
In part two, I will discuss the combo therapy approach.
Dr. Jeffrey Tucker practices in West Los Angeles, California. Visit his website at www.DrJeffreyTucker. com
References:
1. Speed C (2004). Low back pain. BMJ 328 (7448): 1119-21.
2. Deville WL, van der Windt DA, Dzaferagic A, Bezemer PD, Bonier LM (2000). The test of Lasegue: systematic review of the accuracy in diagnosing herniated discs. Spine 25 (9): 1140-7.
3. Br J Sports Med 2019. 53:1464-1473
4. Afonso J et. al. (2021). “he Hamstrings: Anatomic and Physiologic Variations and Their Potential Relationships With Injury Risk, Front Physiol 2021; 12.