by Christine Foss MD, DC, MS.ED., ATC, DACBSP, DACRB, ICSC
The Kinetic Chain is best described as a series of independent systems that work in synchronicity to enable movement. Working at its best, the Kinetic Chain functions to reduce load and create a biomechanically enhanced flow of movement. However, what happens when this system fails? How can we, as practitioners, hack the system and fully understand the WHY of injury to get better and more longstanding patient outcomes?
Ninad Karandikar, in his work “Kinetic Chains: A Review of the Concept and Its Clinical Applications”(1), describes the Kinetic Chain as the movement of a joint that produces predictable movement patterns to local and regional structures. This trending topic is particularly interesting to those health care practitioners who treat the body for maximal global benefit in addition to stopping the volley of cyclic pain and dysfunction.
Evaluation of the Kinetic Chain gives the practitioner the ability to dive into the compensatory patterns that give us a better understanding of performance, injury predisposition, and expedition from injury. Moreover, the Kinetic Chain explains the WHY of injury. This is the most critical correction we can make when treating a patient, moving away from a local-only approach to injury care and looking to the core cause of injury. This core component of injury predisposition or redundancy can then be addressed as part of the patient care plan in recovery and return to activity.
Beginning with compensatory patterns, we must first look at the feet. Evaluation of the feet gives us a human cheat sheet into the hierarchy of patterned use that the body has adopted as normal. Simply put, the foundational faults are easily transferred up to the knees, pelvis, and spine. It’s important to remember that the body generally prefers to prioritize the amount of movement over the quality of it, will instinctively avoid movement that causes pain, and naturally opts for the easiest route for carrying out a motion or bearing weight. By studying these adaptations, we can identify and analyze the underlying causes of injury.
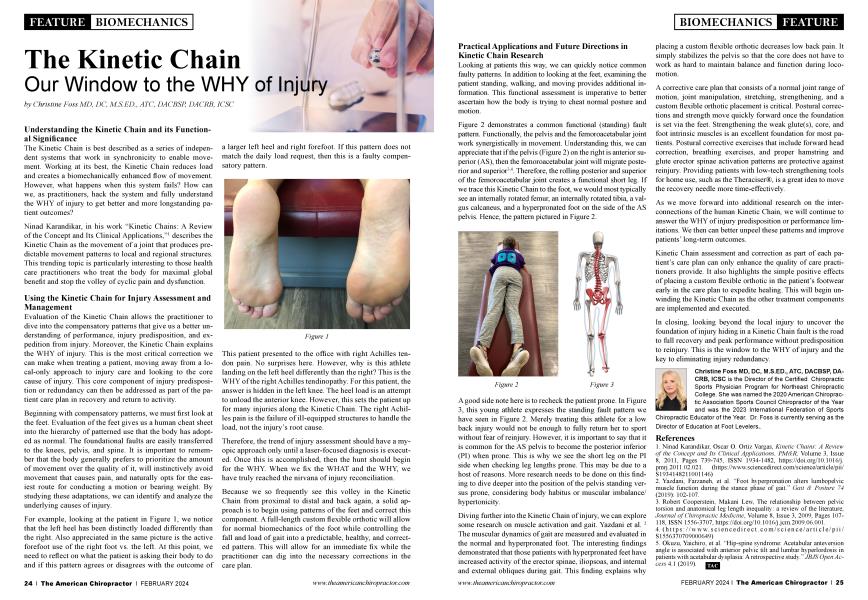
For example, looking at the patient in Figure 1, we can notice that the left heel has been distinctly loaded differently than the right. Also appreciating in the same picture is the active forefoot use of the right foot vs. the left. It is at this point that we need to reflect on what the patient is asking their body to do and if this pattern agrees or disagrees with the outcome of a larger left heel and right forefoot. If this pattern does not match the daily load request, then this is a faulty compensatory pattern.

This patient presented to the office with right Achilles tendon pain. No surprises here. But why is this athlete landing on the left heel differently than the right? This is the WHY of the right Achilles tendinopathy. For this patient, the answer is hidden in the left knee. The heel load is an attempt to unload the anterior knee. However, this sets the patient up for a host of injuries along the Kinetic Chain. The right Achilles pain is the failure of ill-equipped structures to handle the load and not the root cause of the injury.
Therefore, the trend of injury assessment should have a myopic approach only until a laser-focused diagnosis is executed. Once this is accomplished, then the hunt should begin for the WHY. When we fix both the WHAT and the WHY, we have truly reached the Nirvana of injury reconciliation.
Because we so frequently see this volley in the Kinetic Chain from proximal to distal and back again, a solid approach is to begin with the use of patterns of the feet and correct this component. A full-length custom flexible orthotic will allow for normal biomechanics of the foot while controlling the fall and load of gait into a predictable, healthy, and corrected pattern. This will allow for an immediate fix while the practitioner can dig into the corrections needed in the plan of care.
Looking at patients this way, we can quickly notice common faulty patterns. In addition to looking at the feet, examining the patient standing, walking, and moving provides additional information. This functional type of assessment is imperative to ascertain better how the body is trying to cheat normal posture and motion.
Figure 2 demonstrates a common functional (standing) fault pattern. Functionally, the pelvis and the femoroacetabular joint work synergistically in movement. Understanding this, we can appreciate that if the pelvis (Figure 2) on the right is anterior superior (AS), then the femoroacetabular joint will migrate posterior and superior(3,4). The rolling posterior and superior of the femoroacetabular joint, therefore, creates a functional short leg. If we were to trace this Kinetic Chain to the foot, we would most typically see an internally rotated femur, an internally rotated tibia, a valgus calcaneus, and a hyperpronated foot also on the side of the AS pelvis. Hence, the pattern pictured in Figure 2.


A good side note here is to recheck the patient prone. In Figure 3, this young athlete expresses the standing fault pattern we have seen in Figure 2. Just treating this athlete for a low back injury would not be enough to fully return her to sport without fear of reinjury. However, it is important to say that it is not uncommon for the AS pelvis to become the posterior inferior (PI) when prone. This speaks to why we see the short leg on the PI side when checking leg lengths prone. This may be due to a host of reasons. More research needs to be done on this finding to dive deeper into the position of the pelvis standing versus prone, considering body habitus or muscular imbalance/hypertonicity.
Diving further into the Kinetic Chain of injury, we can explore some research on muscle activation and gait. Yazdani et al. (2) The muscular dynamics of gait are measured and evaluated in the normal and hyperpronated foot. The interesting findings demonstrated that those patients with hyperpronated feet have increased activity of the erector spinae, iliopsoas, and internal and external obliques during gait. This explains why placing a custom flexible orthotic decreases low back pain. It simply stabilizes the pelvis so that the core does not have to work as hard to maintain balance and function during locomotion.
A corrective care plan that consists of normal joint range of motion, joint manipulation, stretching, and strengthening, in addition to the placement of a custom flexible orthotic, is critical. Once the foundation is set via the feet, postural corrections and strength move quickly forward. Strengthening the weak glute(s), core, and foot intrinsic muscles is an excellent foundation for most patients. Postural corrective exercises that include forward head correction, breathing exercises, and proper hamstring and glute erector spinae activation patterns are protective against reinjury. Providing patients with low-tech strengthening tools for home use, such as the Theraciser®, is a great idea to move the recovery needle in a more time-effective way.
As we move forward into additional research on the interconnections of the human Kinetic Chain, we will continue to answer the WHY of injury predisposition or performance limitations. We then can better unpeel these patterns and improve patient long-term outcomes.
Kinetic Chain assessment and correction as part of each patient’s care plan can only enhance the quality of care we, as practitioners, provide. It also highlights the simple positive effects of placing a custom flexible orthotic in the patient’s footwear early in the care plan to expedite healing. This will begin the unwinding of the Kinetic Chain as the other treatment components are put into place and executed.
In closing, looking beyond the local injury to uncover the foundation of injury that may be hiding in a Kinetic Chain fault is the road to full recovery and peak performance without predisposition to reinjury. This is the window to the WHY of injury and, moreover, the key to eliminating injury redundancy.
Ninad Karandikar, Oscar O. Ortiz Vargas, Kinetic Chains: A Review of the Concept and Its Clinical Applications, PM&R, Volume 3, Issue 8, 2011, Pages 739-745, ISSN 1934-1482, https://doi.org/10.1016/j.pmrj.2011.02.021. (https://www.sciencedirect.com/science/article/pii/S1934148211001146)
Yazdani, Farzaneh, et al. "Foot hyperpronation alters lumbopelvic muscle function during the stance phase of gait." Gait & Posture 74 (2019): 102-107.
Robert Cooperstein, Makani Lew, The relationship between pelvic torsion and anatomical leg length inequality: a review of the literature, Journal of Chiropractic Medicine,
Volume 8, Issue 3, 2009, Pages 107-118, ISSN 1556-3707, https://doi.org/10.1016/j.jcm.2009.06.001.
(https://www.sciencedirect.com/science/article/pii/S1556370709000649)
Okuzu, Yaichiro, et al. "Hip-spine syndrome: Acetabular anteversion angle is associated with anterior pelvic tilt and lumbar hyperlordosis in patients with acetabular dysplasia: A retrospective study." JBJS Open Access 4.1 (2019).