English has silent letters. I am unsure that a word is more flamboyant, understandable, or improved with a silent k, p, or g — knowledge, knee, psychology, ptarmigans, gnat, and many more.
When speaking, we easily glide past the need to include these letters, but they are non-negotiable and present. Ask any wrinkled, gnarly knave.
Diseases begin silently without symptoms. Over time, the silence may lead to hypertension, atherosclerosis, or osteoporosis. The silence ends with stroke, heart attack, or fractures.
The questions to be asked are: How do we recognize a silent disease? How do we initiate preventive strategies so that the disease does not progress from silent to overt?
Natural Progression
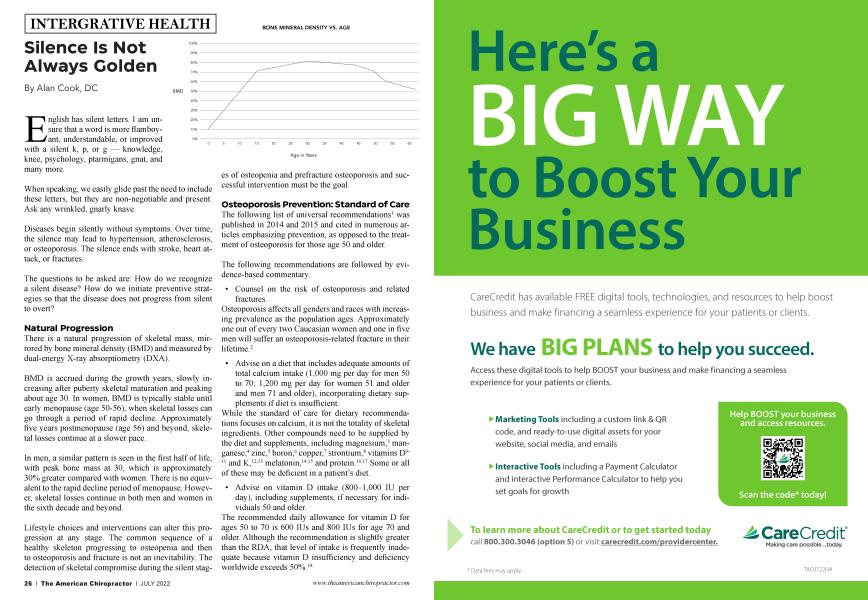
There is a natural progression of skeletal mass, mirrored by bone mineral density (BMD) and measured by dual-energy X-ray absorptiometry (DXA).
BMD is accrued during the growth years, slowly increasing after puberty skeletal maturation and peaking about age 30. In women, BMD is typically stable until early menopause (age 50-56), when skeletal losses can go through a period of rapid decline. Approximately five years postmenopause (age 56) and beyond, skeletal losses continue at a slower pace.
In men, a similar pattern is seen in the first half of life, with peak bone mass at 30, which is approximately 30% greater compared with women. There is no equivalent to the rapid decline period of menopause. However, skeletal losses continue in both men and women in the sixth decade and beyond.
Lifestyle choices and interventions can alter this progression at any stage. The common sequence of a healthy skeleton progressing to osteopenia and then to osteoporosis and fracture is not an inevitability. The detection of skeletal compromise during the silent stages of osteopenia and prefracture osteoporosis and successful intervention must be the goal.
Osteoporosis Prevention: Standard of Care
The following list of universal recommendations1 was published in 2014 and 2015 and cited in numerous articles emphasizing prevention, as opposed to the treatment of osteoporosis for those age 50 and older.
The following recommendations are followed by evidence-based commentary.
• Counsel on the risk of osteoporosis and related fractures.
Osteoporosis affects all genders and races with increasing prevalence as the population ages. Approximately one out of every two Caucasian women and one in five men will suffer an osteoporosis-related fracture in their lifetime.2
• Advise on a diet that includes adequate amounts of total calcium intake (1,000 mg per day for men 50 to 70; 1,200 mg per day for women 51 and older and men 71 and older), incorporating dietary supplements if diet is insufficient.
While the standard of care for dietary recommendations focuses on calcium, it is not the totality of skeletal ingredients. Other compounds need to be supplied by the diet and supplements, including magnesium,3 manganese,4 zinc,5 boron,6 copper,7 strontium,8 vitamins D9' 11 and K,1213 melatonin,1415 and protein.1617 Some or all of these may be deficient in a patient’s diet.
• Advise on vitamin D intake (800-1,000 IU per day), including supplements, if necessary for individuals 50 and older.
The recommended daily allowance for vitamin D for ages 50 to 70 is 600 IUs and 800 IUs for age 70 and older. Although the recommendation is slightly greater than the RDA, that level of intake is frequently inadequate because vitamin D insufficiency and deficiency worldwide exceeds 50%.18
..."For example, too often, the exercise advice gets watered down to “any activity is beneficial,” rather than a specified level of vigor, distance, and frequency."...
Other medical guidelines suggest 1,500 to 5,000 IUs per day for those over 50 years. This enormous discrepancy is a partial explanation for the high rates of osteoporosis.19
Vitamin D can be obtained via diet, supplements, or sunshine on exposed skin. Rather than focusing solely on dietary or supplemental intakes, the more important variable is blood levels. Despite controversies about vitamin D and extra-skeletal functions, there is widespread agreement that blood levels should not go below 30 ng/ml to maintain bone health.
• Recommend regular weight-bearing and muscle-strengthening exercise to improve agility, strength, posture and balance; maintain or improve bone strength; and reduce the risk of falls and fractures.
This is a good recommendation, but the omission of details is important to consider. Specific activities such as volleyball, dance, tai chi, etc., must be customized for a patient’s interest and abilities.
• Assess risk factors for falls and offer appropriate modifications (e.g., home safety assessment, balance-training exercises, correction of vitamin D insufficiency, avoidance of central nervous system depressant medications, careful monitoring of antihypertensive medication, and visual correction when needed).
Those are all important to prevent fracture-inducing falls. Balance, vision, vitamin D insufficiency/deficiency, substance use, and medications that can impair equilibrium and affect fall and fracture risk.
• Advise on cessation of tobacco smoking and avoidance of excessive alcohol intake.
Tobacco affects bone mineral by several mechanisms, including speeding the breakdown of estrogen. Also, smokers tend to have decreased physical activity, which decreases calcium absorption, and resistance to calcitonin (which suppresses bone resorption).20
The use of excessive alcohol can displace good nutrition and impair liver function (necessary for the activation of vitamin D).21
Conclusion
To be serious about the prevention of osteoporosis from the silent to overt stage, we must emphasize the importance of real lifestyle and natural compound interventions. The previously mentioned set of recommendations attempts to address many factors needed to prevent the progression of a healthy skeleton to osteopenia, osteoporosis, and the fractures of the hip, distal forearm, and spine. The discussed lifestyle issues of diet, exercise, calcium and vitamin D, avoidance of tobacco and excessive alcohol, and cautions regarding central nervous system depressant medications are all sensible.
It’s important to exceed these recommendations and include more comprehensive dietary and exercise interventions. For example, too often, the exercise advice gets watered down to “any activity is beneficial,” rather than a specified level of vigor, distance, and frequency. Dietary advice must include attention to nutrients beyond calcium. The ubiquitous consumption of highly processed and sugar-added foods displaces the necessary trace minerals, vitamins, and protein required to build and maintain a skeleton. People need to be reminded to eat real food.
Small tweaks to a patient’s lifestyle often yield no measurable gains. Exercise, diet improvements, and natural compounds can be suggested as a token or as a prescription at a proper dose. Prevention strategies in the form of well-rounded recommendations are vital to displace the common belief in and dependence upon the spectrum of osteoporosis medications.
When the sounds of fracturing bones are heard, osteoporosis is not a silent disease.
Alan Cook, DC, has been in practice since 1989. He ran the Osteoporosis Diagnostic Center (1996-2019), participated in four clinical trials, and lectured nationally. He currently works with the Open Door Clinic system in a multidisciplinary setting and provides video-based continuing education with EasyWebCE. To see more of his work, log onto: www.EasyWebCE.com
For references please visit www.bit.ly/4407Cook