Psoas Muscle Inhibition Part 2: Treatment
CLINICAL RESEARCH
Jamie Raymond
DC, CCSP
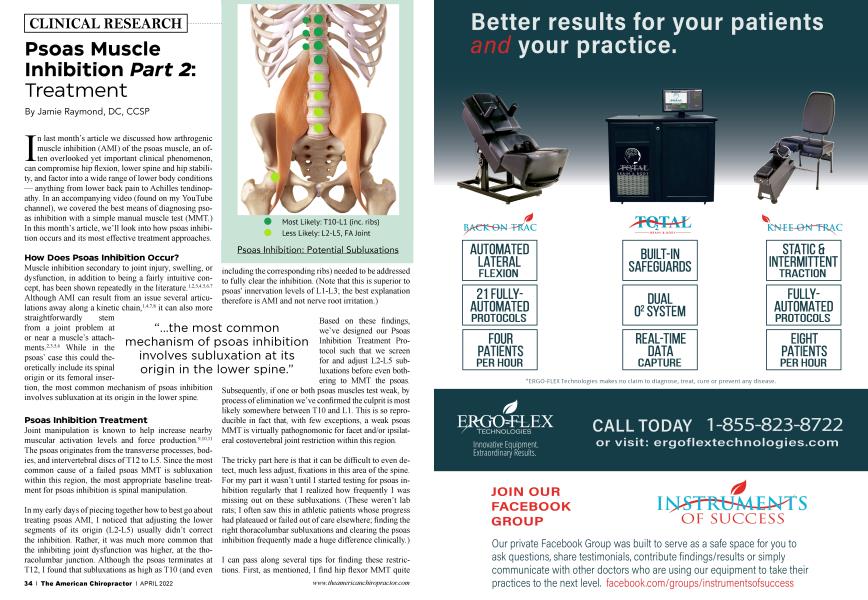
Most Likely: T10-L1 (inc. ribs)
Less Likely: L2-L5, FA Joint
Psoas Inhibition: Potential Subluxations
“...the most common mechanism of psoas inhibition involves subluxation at its origin in the lower spine.”
In last month’s article we discussed how arthrogenic muscle inhibition (AMI) of the psoas muscle, an often overlooked yet important clinical phenomenon, can compromise hip flexion, lower spine and hip stability, and factor into a wide range of lower body conditions — anything from lower back pain to Achilles tendinopathy. In an accompanying video (found on my YouTube channel), we covered the best means of diagnosing psoas inhibition with a simple manual muscle test (MMT.) In this month’s article, we’ll look into how psoas inhibition occurs and its most effective treatment approaches.
How Does Psoas Inhibition Occur?
Muscle inhibition secondary to joint injury, swelling, or dysfunction, in addition to being a fairly intuitive concept, has been shown repeatedly in the literature.L2-3’4-5-6 7 Although AMI can result from an issue several articulations away along a kinetic chain,1A7-8 it can also more straightforwardly stem from a joint problem at or near a muscle’s attachments. 2-3-5’6 While in the psoas’ case this could theoretically include its spinal origin or its femoral insertion, the most common mechanism of psoas inhibition involves subluxation at its origin in the lower spine.
Psoas Inhibition Treatment
Joint manipulation is known to help increase nearby muscular activation levels and force production.91011 The psoas originates from the transverse processes, bodies, and intervertebral discs of T12 to L5. Since the most common cause of a failed psoas MMT is subluxation within this region, the most appropriate baseline treatment for psoas inhibition is spinal manipulation.
In my early days of piecing together how to best go about treating psoas AMI, I noticed that adjusting the lower segments of its origin (L2-L5) usually didn’t correct the inhibition. Rather, it was much more common that the inhibiting joint dysfunction was higher, at the thoracolumbar junction. Although the psoas terminates at T12,1 found that subluxations as high as T10 (and even including the corresponding ribs) needed to be addressed to fully clear the inhibition. (Note that this is superior to psoas' innervation levels of L1-L3; the best explanation therefore is AMI and not nerve root irritation.)
Based on these findings, we’ve designed our Psoas Inhibition Treatment Protocol such that we screen for and adjust L2-L5 subluxations before even bothering to MMT the psoas. Subsequently, if one or both psoas muscles test weak, by process of elimination we’ve confirmed the culprit is most likely somewhere between T10 and LI. This is so reproducible in fact that, with few exceptions, a weak psoas MMT is virtually pathognomonic for facet and/or ipsilateral costovertebral joint restriction within this region.
The tricky part here is that it can be difficult to even detect, much less adjust, fixations in this area of the spine. For my part it wasn’t until I started testing for psoas inhibition regularly that I realized how frequently I was missing out on these subluxations. (These weren’t lab rats; I often saw this in athletic patients whose progress had plateaued or failed out of care elsewhere; finding the right thoracolumbar subluxations and clearing the psoas inhibition frequently made a huge difference clinically.)
I can pass along several tips for finding these restrictions. First, as mentioned, I find hip flexor MMT quite sensitive and specific for T10-L1 subluxation. Consequently, when a psoas muscle tests weak, you have a high degree of certainty you will find a subluxation there. That’s half the battle for any adjustment — feeling confident that there is a restriction to thrust into.
Secondly, it is often easier to find lower thoracic subluxations with the patient supine, as they tend to stand out more, both to the doctor and the patient. Palpating laterally into the lower rib margins is also helpful; rib restrictions are often more tender to touch than spinal joint restrictions. I’ll find the most tender rib or two, then track it back medially to the corresponding vertebrae. I do this all statically, as I find it a bit more precise than motion palpation. It saves me some labor, and I’m also then in position to deliver the supine adjustment (discussed in a moment.) However, if you are more comfortable with motion palpation then by all means find them that way.
Lastly, prone adjusting by itself often isn’t sufficient to fully release a restricted thoracolumbar junction and activate an inhibited psoas. In my first few years of practice, I was quite happy to get any cavitation out of this region of the spine with standard prone adjusting, and if I did, I would call it a success. Later, as I did more psoas MMT, I realized that often prone and supine adjusting were required to fully clear the inhibition. (I believe this is because it is difficult to generate the amount of spinal flexion required when patients are prone.)
“...the most appropriate baseline treatment for psoas inhibition is spinal manipulation.”
The supine adjustment that I adapted was a modified version of one that, ironically, I had learned in chiropractic college but had given up on as being too difficult. I call it the “supine sit-up move.” With the help of colleagues, I’ve spent the past 10 years perfecting this adjustment and simplifying its learning curve to the point that I even successfully taught it to my 19-year-old daughter (she only has one patient — me!)
The supine sit-up move has several other advantages over prone adjusting (and can even be applied superior to the thoracolumbar region, as high as around T6.)
• You are utilizing gravity and the patient’s mass to generate much of the force, typically allowing for bigger cavitations. This includes any costovertebral restrictions, which are difficult to adjust prone.
• The patient is asked to maintain a firmly taught flexed position, which is easier for them than trying to relax for a prone move, when they are anticipating a thrust. When performed correctly, the supine situp move is usually surprisingly comfortable.
• In patients where rib fractures are a concern (e.g., osteopenic individuals), the ribs are better protected in the supine move than when prone.
On my YouTube channel, you can find a video detailing the supine sit-up adjustment. If you haven’t already watched it, check out the video on psoas MMT first. Before attempting this move, you’ll want to establish that the psoas is inhibited, and if so, unilateral or bilateral.
In the last article in this series next month, we’ll discuss the thoracolumbar soft-tissue mobility and stability considerations that frequently play a role in posas-inhibiting subluxations. These soft-tissue findings usually need to be addressed to allow for your adjustments to hold, for the psoas to stay activated, and for whatever injury the psoas inhibition is factoring into to truly resolve.
Jamie Raymond, DC, is a Certified Chiropractic Sports Physician and researcher with more than 20 years of clinical experience. He specializes in the causes and effects of muscle inhibition as it pertains to musculoskeletal injury and has developed innovative protocols to help other providers incorporate best practice treatments to tackle their most difficult cases. Check him out on his YouTube channel.
References
1. Bullock-Saxton JE, Janda If Bullock MI. The influence of ankle sprain injury on muscle activation during hip extension, hit J Sports Med. 1994 Aug; 15(6):3304. dot: 10.1055/S-2007-1021069. PMID: 7822072.
2. McVey ED, Palmieri RM, Docherty CL, Zinder SM, Ingersoll CD. Arthrogenic muscle inhibition in the leg muscles of subjects exhibiting functional ankle instability. Foot Ankle hit. 2005 Dec;26(12):1055-61.
3. Palmieri-Smith RM, Krembrink J, Ashton-Miller JA, Wojtys EM. Quadriceps inhibition induced by an experimental knee joint effusion affects knee joint mechanics during a single-legged drop landing. Am J Sports Med. 2007 Aug;35(8):1269-75.
4. Sedory EJ, McVey ED, Cross KM, Ingersoll CD, Hertel J. Arthrogenic muscle response of the quadriceps and hamstrings with chronic ankle instability. J Athl Train. 2007;42(3):355-360.
5. Palmieri-Smith RM, Hopkins JT, Brown TN. Peroneal activation deficits in persons with functional ankle instability. Am J Sports Med. 2009 May;37(5) :9828.
6. Freeman S, MasciaA, McGill S. Arthrogenic neuromusculature inhibition: a foundational investigation of existence in the hip joint. Clin Biomech (Bristol, Avon). 2013 Feb;28(2):171-7.
7. Jaber H, Lohman E, Daher N, Bains G, Nagaraj A, Mayekar R Shanbhag M, Alameri M. Neuromuscular control of ankle and hip during performance of the star excursion balance test in subjects with and without chronic ankle instability. PLoS One. 2018 Aug 13;13(8):e0201479.
8. Lawrence MA, Raymond JT, Look AE, Woodard NM, Schicker CM, Swanson BT. Effects of tibiofibular and ankle joint manipulation on hip strength and muscle activation. J Manipulative Physiol Ther 2020 Jun;43(5):406-417.
9. Cleland JA, Selleck B, Stowell T, Browne L, Albermi S, St. Cyr H, Caron T. (2004). Short-term effects of thoracic manipulation on lower trapezius muscle strength. Journal of Manual & Manipulative Therapy, 12, 82 - 90.
10. Grindstaff TL, Beazell JR, Sauer LD, Magrum EM, Ingersoll CD, Hertel J. Immediate effects of a tibiofibular joint manipulation on lower extremity H-reflex measurements in individuals with chronic ankle instability. J Electromyogr Kinesiol. 2011 Aug;21(4):652-8. dot: 10.1016j.jelekin. 2011.03. OIL Epub 2011 May 4. PMID: 21546263.
11. Silva Neto JB, Ismania C, de Freitas DG, Cazarini C Jr, Martin RL, Fukuda TY. The effect of a single high velocity low amplitude hip mobilization on strength in subjects with knee injuries. Musculoskelet Set Pract. 2019 Dec;44:102051.