Comprehensive Examination and Correction of the Pelvis
TECHNIQUE
Part One of a Two-Part Series: The Examination
William H. Koch
DC
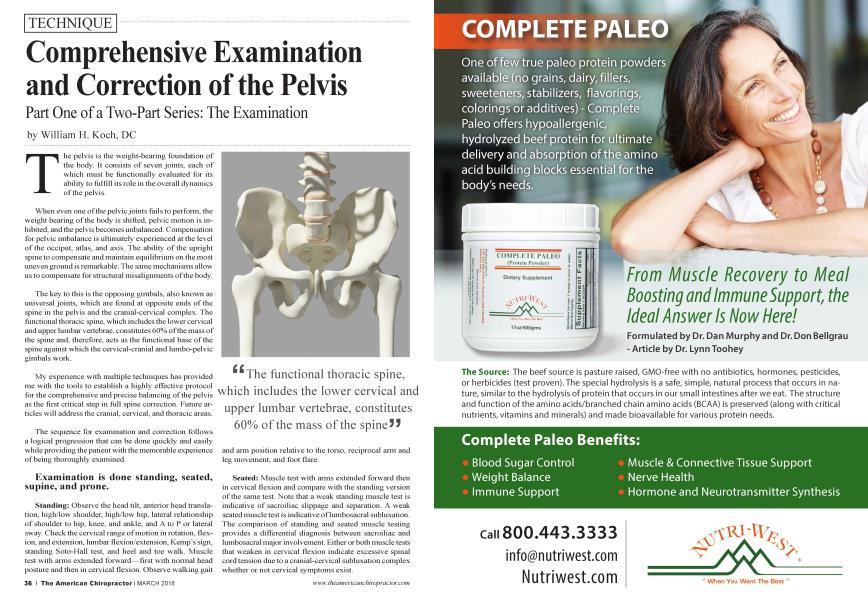
The pelvis is the weight-bearing foundation of the body. It consists of seven joints, each of which must be functionally evaluated for its ability to fulfill its role in the overall dynamics of the pelvis.
When even one of the pelvic joints fails to perform, the weight bearing of the body is shifted, pelvic motion is inhibited, and the pelvis becomes unbalanced. Compensation for pelvic imbalance is ultimately experienced at the level of the occiput, atlas, and axis. The ability of the upright spine to compensate and maintain equilibrium on the most uneven ground is remarkable. The same mechanisms allow us to compensate for structural misalignments of the body.
The key to this is the opposing gimbals, also known as universal joints, which are found at opposite ends of the spine in the pelvis and the cranial-cervical complex. The functional thoracic spine, which includes the lower cervical and upper lumbar vertebrae, constitutes 60% of the mass of the spine and, therefore, acts as the functional base of the spine against which the cervical-cranial and lumbo-pelvic gimbals work.
My experience with multiple techniques has provided me with the tools to establish a highly effective protocol for the comprehensive and precise balancing of the pelvis as the first critical step in full spine correction. Future articles will address the cranial, cervical, and thoracic areas.
The sequence for examination and correction follows a logical progression that can be done quickly and easily while providing the patient with the memorable experience of being thoroughly examined.
Examination is done standing, seated, supine, and prone.
Standing: Observe the head tilt, anterior head translation, high/low shoulder, high/low hip, lateral relationship of shoulder to hip, knee, and ankle, and A to P or lateral sway. Check the cervical range of motion in rotation, flexion, and extension, lumbar flexion/extension, Kemp’s sign, standing Soto-Hall test, and heel and toe walk. Muscle test with arms extended forward—first with normal head posture and then in cervical flexion. Observe walking gait and arm position relative to the torso, reciprocal arm and leg movement, and foot flare.
^The functional thoracic spine, which includes the lower cervical and upper lumbar vertebrae, constitutes 60% of the mass of the spine JJ
Seated: Muscle test with arms extended forward then in cervical flexion and compare with the standing version of the same test. Note that a weak standing muscle test is indicative of sacroiliac slippage and separation. A weak seated muscle test is indicative of lumbosacral subluxation. The comparison of standing and seated muscle testing provides a differential diagnosis between sacroiliac and lumbosacral major involvement. Either or both muscle tests that weaken in cervical flexion indicate excessive spinal cord tension due to a cranial-cervical subluxation complex whether or not cervical symptoms exist.
Supine: Begin with straight leg lift, Lasegue’s, Braggard’s, FABER (Patrick’s), and Soto-Hall tests.
Next is the leg check. Because leg-check accuracy is critical to all procedures that follow, care must be taken to ensure it is observed and recorded correctly. First, the doctor aligns the patient on the table, and then standing at the foot of the table, he or she aligns with the patient. Left and right knees are individually flexed to the chest and then brought back to straight. Leg length difference is carefully observed and measured at the point where the upper part of the shoe joins the sole at the heel. Also, compare the levels of the right and left internal malleolus.
Check for uneven psoas contraction by extending both arms superiorly with palms together and fingers extended. The short side indicates excessive contraction on that side and usually corresponds to the short leg side. Psoas contraction on the side opposite of the short leg indicates a counter torque of upper to lower body. (See my October 2017 TAC article on the psoas.)
Next, check the stability of the symphysis pubis. Both knees are brought up with feet planted on the table. The doctor challenges the patient’s ability to hold knees tightly together. Inability or weakness is indicative of instability of the pubic joint. This will compromise the entire stability of the pelvis.
Anterior femur heads are evaluated by raising each leg individually to 45 degrees and challenging the ability to hold the leg up firmly against downward pressure. Inability to hold leg firmly is indicative of weakness of anterior femur head mechanoreceptors and hip flexors.
L5/S1 facet joints are tested by raising each leg individually to 45 degrees and laterally 45 degrees and challenged in that position. Weakness is indicative of facet imbrication or jamming.
SOT arm-fossa test for sacroiliac slippage and separation is performed on both left and right. Each arm is held vertically with a locked elbow and muscle-tested as the doctor contracts first the upper and then the lower fossa above and below the inguinal ligament midway between the ASIS and the pubic arch. Weakness of any or all fossas is a positive indication of SOT category-two slippage and separation of the sacroiliac joint.
Prone: Prone position allows the doctor to confirm the leg length differential and to do a Deerfield leg check if desired. The posterior femur head mechanoreceptors and leg extensors are evaluated by bending the leg at the knee, lifting it off the table and muscle testing to determine the patient’s ability to lift, and then holding the leg against the doctor’s downward pressure. Inability is indicative of posterior femur head dysfunction and hip extensor weakness.
Muscle testing is not a strength contest but evaluation of a patient’s ability to instantly engage resistance against challenge. When testing the facets, sacroiliacs, and anterior and posterior femur heads, it is important to observe the fine gradations of difference or equality of each paired joint.
Pelvic balance has been achieved when post-correction testing confirms the left and right arm fossas test strong, left and right facets, and anterior and posterior femur heads are bilaterally strong and equal. Finally, the symphysis pubis must test strong. Failure of the pubic joint will destabilize the entire pelvis. Its importance cannot be overstated.
Part two, “The Comprehensive Correction of the Seven Joints of the Pelvis,” will cover corrective protocols appropriate to address positive examination findings and achieve pelvic balance.
Dr. William H. Koch, a 1967 Cum Laude graduate of Palmer College, practiced in The Hamptons, NY ' for 30 years and in The Bahamas for 15 years aboard P ^/ s motor yacht, The Coastal Chiropractor He currently splits his time between A baco, Bahamas and his newest practice in Mount Dora, Florida. Dr. Koch is author of the books “Chiropractic the Superior Alternative ” and Conversations with Chiropractic Technique Masters” available through Amazon.com. He writes a blog: “ChiroPractice Made Perfect ” http: DrWilliamHKoch.com and teaches classes on The Koch Protocols for Integrated Advanced Chiropractic Techniques. He may be contacted via email at outislanddc@drwilliamhkoch. com. Learn more by visiting http://KochSeminars.com.