Current perspectives: AC Separation (Types 1 & 2)
CLINICAL
Cole Hosenfeld
DC, DACBSP
Acromioclavicular (AC) separation can be an enigma to the practicing chiropractor because this injury is not typical of every chiropractic office. As the professions’ specialties broaden and more disciplines team up, shoulder injuries are being treated more often in the chiropractic setting. Documentation of this injury dates back to Hippocrates (460 to 377 BC) and Galen (129 to 199 AD) where concerns about appropriate diagnosis and treatment were noted.1 Science has evolved greatly in the understanding of the shoulder complex, intrinsic injuries, and conservative approaches to management.
The focus of this article is to address type 1 and 2 AC joint separation and their management. There are six types of AC separation with a general consensus to manage types 1 and 2 conservatively; grades 4, 5, and 6 operatively; and grade 3 individually.12
Among the sports and recreational athlete population, AC joint injuries are common, constituting roughly 12% of the injuries of the shoulder. Males tend to have a higher incidence of these injuries, especially those under 30 who participate in a contact sport.12 The mechanism of injury tends to be a fall or collision directly onto the shoulder complex, forcing the scapulohumeral girdle downward abruptly. These are seen in bicycle wrecks, soccer, football, basketball, motorcycle, and motor vehicle accidents.12 4,5,6 This action results in tearing or spraining of the AC ligament and the coracoclavicular (CC) ligaments. Grades 3 through 6 are more likely to have additional structures injured, such as the labrum.
Because the shoulder is a complex joint, it includes the diarthrodial AC joint, which is made of a thin cartilage surface with a fibrocartilaginous meniscoid disk. The surrounding capsule is known as the AC ligament and is combined with the CC ligament, providing resting stability. Movement of the arm through closedand open-packed motions places substantial multiplane forces in the vertical, anteroposterior (A-P), and axial planes of the AC joint complex.
The AC ligament contributes 20 to 50% stability resistance in the superior direction, and 90% stability resistance in the A-P plane. The CC ligaments are made of medial and lateral fibers— conoid and trapezoid, respectively—and provide restriction of the scapulohumeral complex in the inferior and medial plane relative to the clavicle. Dynamic stabilization of the AC joint is provided by the trapezius and deltoid fascia.16
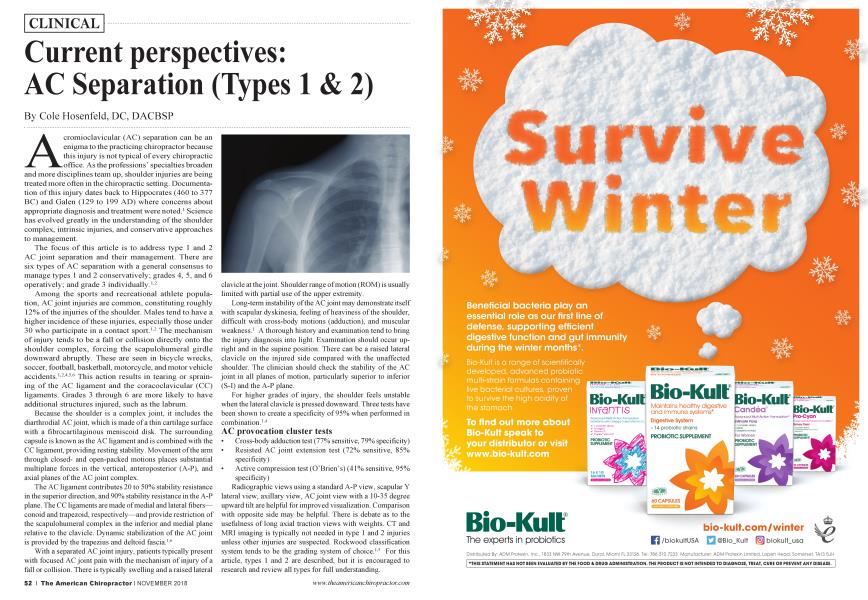
With a separated AC joint injury, patients typically present with focused AC joint pain with the mechanism of injury of a fall or collision. There is typically swelling and a raised lateral clavicle at the joint. Shoulder range of motion (ROM) is usually limited with partial use of the upper extremity.
Long-term instability of the AC joint may demonstrate itself with scapular dyskinesia, feeling of heaviness of the shoulder, difficult with cross-body motions (adduction), and muscular weakness.1 A thorough history and examination tend to bring the injury diagnosis into light. Examination should occur upright and in the supine position. There can be a raised lateral clavicle on the injured side compared with the unaffected shoulder. The clinician should check the stability of the AC joint in all planes of motion, particularly superior to inferior (S-I) and the A-P plane.
For higher grades of injury, the shoulder feels unstable when the lateral clavicle is pressed downward. Three tests have been shown to create a specificity of 95% when performed in combination.1-4
AC provocation cluster tests
• Cross-body adduction test (77% sensitive, 79% specificity)
• Resisted AC joint extension test (72% sensitive, 85% specificity)
• Active compression test (O’Brien’s) (41% sensitive, 95% specificity)
Radiographic views using a standard A-P view, scapular Y lateral view, axillary view, AC joint view with a 10-35 degree upward tilt are helpful for improved visualization. Comparison with opposite side may be helpful. There is debate as to the usefulness of long axial traction views with weights. CT and MRI imaging is typically not needed in type 1 and 2 injuries unless other injuries are suspected. Rockwood classification system tends to be the grading system of choice.1-5 For this article, types 1 and 2 are described, but it is encouraged to research and review all types for full understanding.
Type 1: AC and CC ligaments are intact.15 Type 2: CC ligament is intact. AC ligament is disrupted. (50% vertical clavicular subluxation is noted typically)15 Type 3: AC and CC ligament structures are disrupted15 Type 4: AC and CC ligaments are disrupted. Distal end of clavicle is displaced posteriorly into or through the trapezius muscle. Clavicle and acromion are widely separated.1-5
Type 5: AC and CC ligaments are disrupted. Muscle attachments are disrupted. Clavicle and acromion are widely separated.15
Type 6: AC and CC ligaments are disrupted. The distal clavicle is dislocated inferior to the coracoid process and posterior to the joining tendons.1-5
Generally, types 1 through 3 are treated nonoperatively; however, type 3 surgical options tend to be reserved for highlevel athletes and high-demand occupations, but the long-term success is still debated. 1 Proper early management appears to improve outcomes in this patient population. Acute stage treatment protocols are listed.2
Clinical pearl: Current soft tissue injury management avoids NS AID use unless absolutely necessary for these injuries as the medication has been shown to slow healing and has poor side effects.3
Acute stage: Type 1 (Days 1 through 7)2
• Ice
• Healthy eathig using anti-inflammatory concepts, high water intake (throughout injury and beyond)
• Side sleepers: hug a pillow
• Leulcotape or lc-tape AC joint for stability of AC joint
• Tylenol (if needed)
• Shoulder sling five to seven days; rest as needed
• AROM: fingers, wrist, elbow
• Day 3: Begin pendulum exercises
• Day 3: Shoulder isometrics including deltoid and trapezius
• Day 3: Add heat/ice contrast therapy Acute stage: Type 1 (Days 7 through 10)2
• Expect symptoms to subside
• Discontinue sling
• Type 1 can progress to ROM and strengthening as symptoms allow.
• Type 1 can return to sport or work when normal ROM and strength obtained. No heavy lifting or contact sports until full, painless ROM and no point tenderness over AC joint.
• Estimated healing time is three weeks. Some have persistent symptoms and surgery can occur in later years secondaiy to degenerative changes.
Acute stage: Type 2 (Days 1 through 7)2
• Ice
• Healthy eating using anti-inflammatory concepts, high water intake (throughout injury and beyond)
• Side sleepers: hug a pillow
• Leulcotape or lc-tape AC joint for stability of AC joint
• Tylenol (if needed)
• AROM: fingers, wrist, elbow
• Shoulder sling seven to 14 days; rest as needed Acute stage: Type 2 (Days 7 through 14)2
• Gentle ROM for shoulder
• Begin pendulum exercises
• Allow use of arm for ADL
• Discontinue sling seven to 14 days
• AROM and strengthening as symptoms allow Acute stage: Type 2 (Days > than 14)2
• Type II can return to sport or work when normal ROM and strength obtained. No heavy lifting or contact sports until full, painless ROM and no point tenderness over AC joint
• Estimated healing time is six weeks plus. Like type 1, some have persistent symptoms and surgery can occur in later years secondary to degenerative changes.
The goal of in-office treatment is pain relief to reduce reinjury, achieve improved ROM/joint play, improve strength, maximize posture, functional independence, independent home exercise program, and return to vocation or sport. Treatment in the clinic typically is one or two times per week for four weeks after the initial acute phase for you and your team of clinical therapy assistants. It is important to relay to your team, who will be integral in the application of your directions, about how the injury care plan should be delivered.
Focus of visits is typically patient education, progression horn PROM to AAROM to AROM, posture exercises, and focused strengthening on the trapezius, deltoid, rotator cuff, and scapular musculature. These exercises can include isometrics, seated press-ups, side-lying external rotation, scaption strengthening, forward flexion strengthening, push-ups, and exercise bands. Manual care includes adjustments to the cervical and thoracic regions and mobilization to the scapula and glenohumeral joint (not the AC joint).2 Modalities are a benefit as needed, including cold laser, electrical stimulation, and thermal therapies.
With a better understanding of acromioclavicular separation, the chiropractic physician will be equipped to detect and manage the injury when it does present in the practice, and clinically educated assistants can play a key role in the positive outcome. A well-trained team flees you up to examine and treat a wide variety of conditions and people in a more effective manner.
References:
1. Van Bergen et al. New insights in the treatment of acromioclavicular separation. World J Orthop. 2017 ; December 18; 8(12): 861-873
2. Standard of Care: Acromioclavicular Joint Separation; The Brigham and Women's Hospital. Inc. Department of Rehabilitation Services; https://www.brighamandwomens.org/.../shoulderacromioclavicular-separation.pdf Accessed August 5, 2018
3. Lippi Gl, Franchini M, Guidi GC, Kean WF., Non-steroidal anti-inflammatory drugs in athletes. Br J Sports Med. 2006 Aug;40(8):661-2; discussion 662-3.
4. Chronopoulos E, Kim TK, Park HB, Ashenbrenner D, McFarland EG. Diagnostic value of physical tests for isolated chronic acromioclavicular lesions. Am J Sports Med 2004; 32: 655-661 [PMID: 15090381 DOI: 10.1177/0363546503261723]
5. Rockwood CA. Disorders of the acromioclavicular joint. In: Rockwood CA, Matsen FA, editors. The shoulder. 4th ed. Philadelphia: WB Saunders, 2009: 453-526
6. Mazzocca AD, Spang JT, Rodriguez RR, Rios CG, Shea KP, Romeo AA, Arciero RA. Biomechanical and radiographic analysis of partial coracoclavicular ligament injuries. Am J Sports Med 2008; 36: 1397-1402 [PMID: 18375786 DOI: 10.1177/0363546508315200]
7. Owens BD et al. Acromioclavicular Joint Separations. Available at: http://www.emedicine.com/orthoped/topic462.htm. Accessed August 5, 2018
Hosenfeld, DC, DACBSP, practices in Knoxville, Tennessee. He is board certified in sports medicine and practices in an integrative provider setting with a team of paraprofessionals. He sits on Tennessee's regulatory board and is coauthor of the textbook Chiropractic Therapy Assistant: A Clinical Resource Guide. He can be reached by email at [email protected] or contact by phone at 615-383-6231.