Clinical Corner: Adhesive Capsulitis A Team Approach to Frozen Shoulder is Essential for Strong Outcomes
CLINICAL
Cole Hosenfeld
DC, DACBSP
Mary, age 49, presents to the clinic after calling the front office staff for an urgent appointment Monday morning because she woke up and couldn’t move her shoulder. During her evaluation, she describes that her shoulder has been mildly aggravating over the past few months and has been worsening over the past week, particularly at night, which causes her to take more ibuprofen to try to get comfortable. She denied any form of trauma or prior medical or surgical history of the shoulder.
She describes that yesterday morning she awoke with more shoulder pain and was unable to move her shoulder. She was in obvious distress and fear of what was happening. After a thorough consultation and examination, she was diagnosed with adhesive capsulitis, also known as frozen shoulder, and the previously mentioned presentation is classic to the onset of the condition.
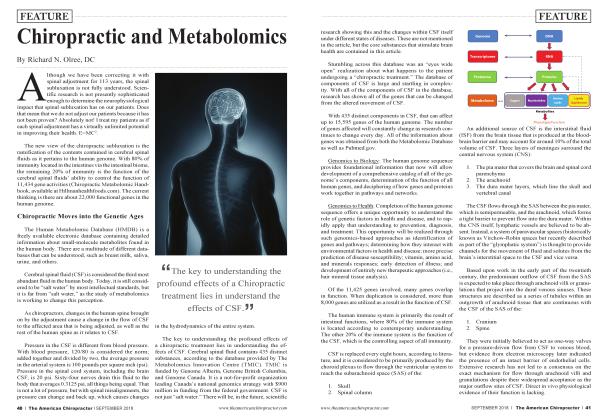
The shoulder joint is a complex structure of bone, joints, ligaments, muscles, bursa sacs, and traversing vasculature, nerves, and lymphatic channels. The offending structure has to do with the strong fibrous capsule surrounding the glenohumeral joint, which connects the scapula and humerus creating the “ball and socket joint.”
The etiology of frozen shoulder is unclear, but it is thought that scar-like adhesion sets up in the capsule, and inflammation is thought to be a key player. It is estimated that between 2 to 5% of the population are affected in their lifetime. Frozen shoulder tends to occur between 40 to 60 years of age with more of a prevalence in women.
Interestingly, up to 20% of diabetics are likely to get frozen shoulder, but the exact mechanism is unknown. Additionally, those who suffer from thyroid disease, have had recent surgery, Parkinson’s, or stroke are more likely to get the disorder, suggesting further evidence of an endocrine and connective tissue connection. Most people who suffer from frozen shoulder only get it once in their lifetime, but as much as 20% of those who had the disorder in one shoulder will get it in the other.
Diagnosis of frozen shoulder by the chiropractic physician is primarily done clinically by examination and history. Difficult cases may require examination with X-rays and MRI or lab testing, but that is often not needed and typically is used to rule out other possible underlying causes, such as labral tears, rotator cuff tears, tumors, impingement syndrome, dislocation, and fracture.
Frozen shoulder can improve on its own without treatment, but it can be painful and take a long time. The condition typically goes through three phases:
• In the first stage, the shoulder starts hurting and becomes increasingly painful. The pain worsens at night when sleeping on the affected shoulder or when the shoulder is flexed, abducted, extended, or externally rotated. This stage typically lasts two to nine months.
• In the second stage, the shoulder locks up or “freezes.” Movement becomes much more limited, but the pain begins to decrease. The shoulder girdle musculature will tend to weaken because of poor range of motion. This stage lasts between four and twelve months.
• In the third stage, the shoulder begins to “thaw,” becoming easier to move and can take one to three years to occur.
Although the condition is self-limiting, chiropractic treatment can be quite helpful in reducing pain and improving mobility within the appropriate phases of care. Orthopedic treatment can be helpful to chiropractic treatment through the use of pain relief interventions and intra-articular steroid injections, which are thought to temporarily “soften” the capsule to allow chiropractic manual intervention to be more effective.
Chiropractors and their clinical assistants are integral to helping these patients heal. Initially and throughout treatment, the chiropractic team helps patients manage their frustrations, helping the patient have proper expectations and a full understanding of life behaviors that influence healing.
From a dietary aspect, focusing on eating habits that are anti-inflammatory from the outset of the injury is helpful, such a paleo diet, and offering recommendations limiting wheat and carbohydrates. Supplementation with omega-3 s, magnesium, turmeric, probiotics, and a quality multivitamin are thought to be helpful by addressing the inflammatory-gut connection, which is gaining increased study as a contributor to inflammatory joint and connective tissue disorders.
Beyond daily living habits and goal expectations, chiropractic treatment focuses on exercises, range of motion, manipulation, mobilization, manual therapies, and therapeutic modalities. Manipulation and mobilization
by the chiropractor seek to restore motion in the cervical spine, thoracic spine, glenohumeral, acromioclavicular, and scapulothoracic areas.
Particular emphasis is placed on the glenohumeral and surrounding capsule where these treatments seek to break up adhesions. The trained chiropractic assistant provides various massage techniques, administers heat and modalities such as laser therapy and ultrasound, and instructs various levels of exercise to improve range of motion.
Exercises are critical to improving range of motion and maintaining strength of the shoulder girdle. Treating the area with manual care techniques and heat prior to exercise is beneficial. Exercises need to push patients out of their comfort zone in order to improve elasticity of the capsule. Placing an emphasis on performing exercises daily is a must.
Exercises beneficial in treating frozen shoulder include:
• Shoulder pendulum exercises.
• Wall walks to increase forward flexion.
• Anterior shoulder stretch through stretching the pectorals.
• Internal rotation behind the back and side-lying.
• Hold broom handle behind back and lift up, which helps stretch the front of the shoulder.
• Hold broom handle in front with elbows at 90 degrees. Slowly shift the handle sideways each direction and hold for 15 seconds to improve external rotation.
• Shoulder shrugs and rolls (up and down and in circles).
• Thoracic extension exercises, such as cat/camel.
The goal of the exercise is to restore flexion/extension, abduction, adduction, and intemal/extemal rotation of the shoulder while also increasing ranges of motion for the cervical and thoracic spines.
In summary, a frozen shoulder can be very disruptive to our patients’ lives. A focus on integral communication and care delivery between the chiropractor and the clinical assistant is essential for strong outcomes and a return to the desired quality of life. An openness to collaboration with other disciplines will further aid in functional restoration and pain reduction.
Initially, educate the patient about the nature of the disorder and review dietary and daily behaviors. Progress to manual care interventions, including manipulation, mobilization, exercise rehabilitation, and timely administration of therapeutic modalities. In conjugation, this multimodal approach can provide the desired outcome your patient is seeking.
References:
1. Tashjiicm RZ. The effectiveness of non operative treatment for frozen shoulder: a systematic review. Clin J Sport Med. 2012, Mar; 22 (2): 168-9.
2. Strunce J, et al. The immediate effects of thoracic spine and rib manipulation on subjects with primary complaints of shoidder pain. Journal of Manual & Manipulative Therapy, 2009;17:230-236.
3. Morgan W, Potthoff S. Managing The Frozen Shoidder, Self-care manualfor those suffering from frozen shoulder, Walter Reed National Military Medical Center, Chiropractic Clinic, drmorgan. mfo/data/documents/frozen-shoulderebook.pdf
4. EwaldA. Adhesive capsulitis: a review. Am Fam Physician 2011; 83(4): 417-422. [PubMed]
5. Maund E, Craig D, Suekarran S, Neilson A, Wright K, Brealey S et al. Management of frozen shoulder: a systematic review and cost-effectiveness analysis. Health Technol Assess 2012; 16(11): 1-264. [PMCfree article] [PubMed]
Cole Hosenfeld, DC, DACBSP, practices in Knoxville, Tennessee. He is board certified in sports medicine and practices in an integrative provider setting with a team of paraprofessionals. He sits on Tennessee’s regulatory board and is coauthor of the textbook Chiropractic Therapy Assistant: A Clinical Resource Guide. He can be reached by email at cole@ applehealthwellness.com or contact by phone at 615-383-6231.