The Mechanism of the Chiropractic Spinal Adjustment/Manipulation:
FEATURE
Ligaments and the Bio-Neuro-Mechanical Component
Part Two of a Five-Part Series
Mark Studin
DC, FASBE(C), DAAPM, DAAMLP and William J. Owens, DC, DAAMLP
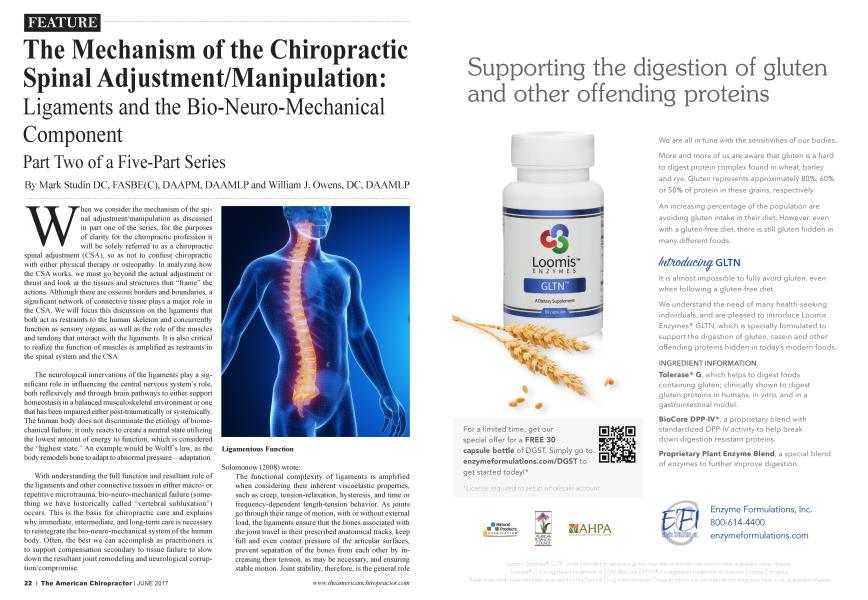
When we consider the mechanism of the spinal adjustment/manipulation as discussed in part one of the series, for the purposes of clarity for the chiropractic profession it will be solely referred to as a chiropractic spinal adjustment (CSA), so as not to confuse chiropractic with either physical therapy or osteopathy. In analyzing how the CSA works, we must go beyond the actual adjustment or thrust and look at the tissues and structures that “frame” the actions. Although there are osseous borders and boundaries, a significant network of connective tissue plays a major role in the CSA. We will focus this discussion on the ligaments that both act as restraints to the human skeleton and concurrently function as sensory organs, as well as the role of the muscles and tendons that interact with the ligaments. It is also critical to realize the function of muscles is amplified as restraints in the spinal system and the CSA.
The neurological innervations of the ligaments play a significant role in influencing the central nervous system’s role, both reflexively and through brain pathways to either support homeostasis in a balanced musculoskeletal environment or one that has been impaired either post-traumatically or systemically. The human body does not discriminate the etiology of biomechanical failure; it only reacts to create a neutral state utilizing the lowest amount of energy to function, which is considered the “highest state.” An example would be Wolff’s law, as the body remodels bone to adapt to abnormal pressure—adaptation.
With understanding the full function and resultant role of the ligaments and other connective tissues in either macroor repetitive microtrauma, bio-neuro-mechanical failure (something we have historically called “vertebral subluxation”) occurs. This is the basis for chiropractic care and explains why immediate, intermediate, and long-term care is necessary to reintegrate the bio-neuro-mechanical system of the human body. Often, the best we can accomplish as practitioners is to support compensation secondary to tissue failure to slow down the resultant joint remodeling and neurological corruption/compromise.
Solomonow (2008) wrote:
The functional complexity of ligaments is amplified when considering their inherent viscoelastic properties, such as creep, tension-relaxation, hysteresis, and time or frequency-dependent length-tension behavior. As joints go through their range of motion, with or without external load, the ligaments ensure that the bones associated with the joint travel in their prescribed anatomical tracks, keep full and even contact pressure of the articular surfaces, prevent separation of the bones from each other by increasing their tension, as may be necessary, and ensuring stable motion. Joint stability, therefore, is the general role
of ligaments without which the joint may subluxate, cause damage to the capsule, cartilage, tendons, nearby nerves and bloodvessels, discs (if considering spinal joints), and to the ligaments themselves. Such injury may debilitate the individual by preventing or limiting his/her use of the joint and the loss of function. Dysfunctional corrupted ligaments, therefore result in a complex-syndrome, various sensory-motor disorders, and other long-term consequences, which impact the individual’s well-being, his athletic activities, employer, skilled workforce pool, and national medical expenses (p. 137)
Ligaments are closely packed collagen fibers that are helical at rest in a crimp pattern. This crimp pattern allows the ligament to recruit other fibers when stressed to support the joint and help prevent ligamentous failure or subfailure (tearing of the ligament). They are comprised of collagen and elastin that give it both tensile strength and elasticity with no two joints alike in composition because each joint has a specific biomechanical role and varies depending upon the needs of that joint.
Image: https://wings.buffalo.edu/eng/mae/courses/417-517/
Solomonow (2008) continued:
As axial stretching of a ligament is applied, fibers or bundles with a small helical wave appearance straighten first and begin to offer resistance (increased stiffness) to stretch. As the ligament is further elongated, fibers or fiber bundles of progressively larger helical wave straighten and contribute to the overall stiffness. Once all the fibers are straightened, a sharp increase in stiffness is observed. Overall, the mostly collagen (75%), elastin, and other substances structure of ligaments is custom tailored by long evolutionary processes to provide various degrees of stiffness at various loads and at various ranges of motion of a joint, while optimally fitting the anatomy inside (inter-capsular) or outside (extra-capsular) a given joint. The various degrees of helical shape of the different fibers allows generation of a wide range of tensile forces by the fiber recruitment process, whereas the overall geometry of the ligament allows selective recruitment of bundles such as to extend function over a wide range of motion. The large content of water (70%) and the cross weave of the long fibers by short fibers provides the necessary lubrication for bundles to slide relative to each other, yet to remain bundled together and
generate stiffness in the transverse directions, (p. 137)
1. Length-tension and recruitment: The general lengthtension (or strain-stress) behavior of a ligament is nonlinear. The initial reports demonstrate rather large strain for very small increase in load. Once all the waves in the collagen fibers of the ligament have been straightened out, and all of the fibers were recruited, additional increase in strain is accompanied with a fast increase in tension.
2. Creep: When a constant load is applied to a ligament, it fust elongates to a given length. If left at the same constant load, it will continue to elongate over time in an exponential fashion up to a finite maximum.
3. Tension-relaxation: When ligaments are subjected to a stretch and hold over time (or constant elongation) the tension-relaxation phenomena is observed. The tension in the ligament increases immediately upon the elongation to a given value. As time elapses, the tension decreases exponentially to a finite minimum while the length does not change.
4. Strain rate: The tension developed hi a ligament also depends on the rate of elongation or strain rate. In general, slow rates of elongation are associated with the development of relatively low tension, whereas higher rates of elongation result hi the development of high tension. Fast stretch of ligaments, such as in high-frequency repetitive motion or in sports activities, are known to result in high incidents of ligamentous damage or rupture. Fast rates
of stretch, therefore, may exceed the physiological loads that could be sustained by a ligament safely, yet it may still be well within the physiological length range. Development of high tension in the ligaments may result in rupture and permanent sensory-motor deficit to the joint in addition to deficit in its structural functions.
Author’s note: A fast strain rate within the physiological lhnit may also cause ligamentous damage as the ligament hasn’t had enough time to adapt (stretch) to its new tensile demand and this is called a “subfailure.”
5. Hysteresis: This phenomenon is associated with repetitive motion when a series of stretch-release cycles are performed over time, (pp. 138-140)
Ligament Reaction to Trauma and Healing
Ligament Inflammation: Inflammatory response in ligaments is initiated whenever the tissue is subjected to stresses which exceed its routine limits at a given time. For example, a sub-injury/failure load, well within the physiological limits of a ligament when applied to the ligament by an individual who does not do that type of physical activity routinely. The normal homeostatic metabolic, cellular, circulatory, and mechanical limits are therefore exceeded by the load, triggering an inflammatory response. Another case where acute inflammation is present is when physical activities presenting sudden overload/stretch cause
a distinct damage to die tissue, which is felt immediately. Such cases, as a sudden loss of balance, a fall, collision with another person, exposure to unexpected load, etc., may result in what is called a sprain injury or a partial rupture of the ligament. Acute inflammation sets in within several hours and may last several weeks and up to 12 months. The healing process, however, does not result in full recovery of the functional properties of the tissue. Mostly, only up to 70% of the ligament’s original structural and functional characteristics are attained by healing post-injury.
Chronic inflammation is an extension of an acute inflammation when the tissue is not allowed to rest, recover, and heal. Repetitive exposure to physical activity and reloading of the ligament over prolonged periods without sufficient rest and recovery represent cumulative microtrauma. The resulting chr onic inflammation is associated with atrophy and degeneration of the collagen matrix leaving a permanently damaged, weak, and non-functional ligament. The dangerous aspect of a chronic inflammation is the fact that it builds up silently over many weeks, months, or years (dependent on presently unknown dose-duration levels of the stressors) and appeals one day as a permanent disability associated with pain, limited motion, weakness, and other disorders. Rest and recovery of as much as two years allows only partial resolution of the disability. Full recovery was never reported, (p. 143)
Dolan et al. (2013) reported that once a ligament is overloaded in either a failure or subfailure, then the tissue fails, resulting in
partial or complete tear known as a sprain. When this occurs, the body “attempts” to repair the damaged ligament, but cannot completely.
They wrote:
With time, the tissue matrix starts to resemble normal ligament tissue; however, critical differences in matrix structure and function persist. In fact, evidence suggests that the injured ligament structure is replaced with tissue that is grossly, histologically, biochemically, and biomechanically similar to seal' tissue, (p. 6)
The persisting abnormalities present in the remodeled ligament matrix can have profound implications on joint biomechanics, depending on the functional demands placed on the tissue. Since remodeled ligament tissue is morphologically and biomechanically inferior to normal ligament tissue, ligament laxity results, causing functional disability of the affected joint and predisposing other soft tissues in and around the joint to further damage, (p. 7)
In fact, studies of healing ligaments have consistently shown that certain ligaments do not heal independently following rupture, and those that do heal, do so with characteristically inferior compositional properties compared with normal tissue. It is not uncommon for more than one ligament to undergo injury during a single traumatic event, (p. 8) Author’s note: Ligaments are made with fibroblast that pro-
duce collagen and elastin and model the ligament throughout puberty. Once puberty is over, the fibroblasts stop producing any ligamentous tissue and remain dormant. Upon injury, the fibroblast activates, but now can only produce collagen, leaving tlie joint stiffer and in a biomechanically compromised functional environment. The above comment verifies that in the literature.
Osteoarthritis [OA] or joint degeneration is one of the most common consequences of ligament laxity. Traditionally, the pathophysiology of OA was thought to be due to aging and wear and teai' on a joint, but more recent studies have shown that ligaments play a crucial role in the development of OA. OA beghis when one or more ligaments become unstable or lax, and the bones begin to track improperly and put pressure on different areas, resulting in the nibbing of bone on cartilage. This causes the breakdown of cartilage and ultimately leads to deterioration, whereby the joint is reduced to bone on bone, a mechanical problem of the joint that leads to abnonnality of the joint’s mechanics. Hypennobility and ligament laxity have become clear risk factors for the prevalence of OA. The results of spinal ligament injury show that over time the inability of the ligaments to heal causes an increase in the degeneration of disc and facet joints, which eventually leads to osteochondral degeneration, (p. 9)
Ligaments as Sensory Organs
Spinal pahi and the effects of the chiropractic spinal adjustment are both central and peripheral in etiology. According
to Studin and Owens (2016), the CSA also affects the central nervous system with systemic sequellae, verifying that chiropractic supports systemic changes and is not solely “back pain providers.” Although chiropractic is not limited to pain, we do treat back pain, inclusive of all spinal regions. Regarding pain, much of the pain generators originate in the ligaments.
Solomonow (2009) wrote:
While ligaments are primarily known for mechanical support for joint stability, they have equally important sensory functions. Anatomical studies demonstrate that ligaments in the extremity joints and the spine are endowed with mechanoreceptors consisting of: Pacinian, Golgi, Ruffini, and bare nerve endings. The presence of such afferents in the ligaments confirms that they contribute to proprioception and kinesthesia, and may also have a distinct role in reflex activation or inhibition of muscular activities, (p. 144)
Chieyeko Tsuchitani, PhD, at the University of Texas reported on all the following receptors, inclusive of the graphics
at: http://neuroscience, uth. tmc. edu/s2/chapter02. html.
Pacinian corpuscles are found in subcutaneous tissue beneath the dermis and in the connective tissues of bone (ligaments and tendons), the body wall, and body cavity. Therefore, they can be cutaneous, proprioceptive, or visceral receptors, depending on their location.
When a force is applied to the tissue overlying the Pacinian corpuscle, its outer laminar cells, which contain fluid, are displaced and distort the axon terminal membrane. If the pressure is sustained on the corpuscle, the fluid is displaced, which dissipates the applied force on the axon terminal. Consequently, a sustained force on the Pacinian corpuscle is transformed into a transient force on its axon terminal. The Pacinian corpuscle la afferent axon response is rapidly adapting, and action potentials are only generated when the force is first applied.
The Ruffini corpuscles are found deep in the skin, as well as in joint ligaments and joint capsules and can function as cutaneous or proprioceptive receptors, depending on their location. The Ruffini corpuscle is cigar-shaped, encapsulated, and contains longitudinal strands of collagenous fibers that are continuous with the connective tissue of the skin or joint. Within the capsule, the la afferent fiber branches repeatedly, and its branches are intertwined with the encapsulated collagenous fibers.
Ruffini corpuscles in skin are considered to be skin-stretch sensitive receptors of the discriminative touch system. They also work with the proprioceptors in joints and muscles to indicate the position and movement of body parts.6
Golgi tendon organs are found in the tendons of striated extrafusal muscles near the muscle-tendon junction Golgi tendon organs resemble Ruffini corpuscles. For example, they are encapsulated and contain intertwining collagen bundles, which are continuous with the muscle tendon, and fine branches of afferent fibers that weave between the collagen bundles. They are functionally “in series” with striated muscle.
The Golgi tendon organ is a proprioceptor that monitors and signals muscle contraction against a force (muscle tension), whereas the muscle spindle is a proprioceptor that monitors and signals muscle stretch (muscle length).
Free nerve endings of la afferents are abundant in muscles, tendons, joints, and ligaments. These free nerve endings are considered to be the somatosensory receptors for pain resulting from muscle, tendon, joint, or ligament damage, and are not considered to be part of the proprioceptive system. These free nerve endings are called nociceptors.
Solomonow (2009) commented:
The presence of such afferents in the ligaments confirms that they contribute to proprioception and kinesthesia, and may also have a distinct role in reflex activation or inhibition of muscular activities. Overall, the decrease or loss of function in a ligament due to rupture or damage does not only compromise its mechanical contributions to joint stability, but also sensory loss of proprioceptive and kinesthetic perception and fast reflexive activation of muscles and the forces they generate in order to enforce joint stability.
It was suggested, as far back as the turn of the last century, that a reflex may exist from sensory receptors in the ligaments to muscles that may directly or indirectly modify the load imposed on the ligament. A clear demonstration of a reflex activation of muscles finally provided in 1987 and reconfirmed several times since then. It was further shown that such a ligamento-muscular reflex exists in most extremity joints and in the spine.
Ligamento-muscular reflexes, therefore, may be inhibitory or excitatory, as may be fit to preserve joint stability; inhibiting muscles that destabilize the joint or increased antagonist co-activation to stabilize the joint.
Spinal Stabilization and Destabilization
Panjabi (2006) reported:
1. Single trauma or cumulative microtrauma causes subfailure injury of the spinal ligaments and injury to the mechanoreceptors (author’s note: and nociceptors) embedded in the ligaments.
2. When the injured spine performs a task or it is challenged by an external load, the transducer signals generated by the mechanoreceptors (author’s note: and nociceptors) are corrupted.
3. Neuromuscular control unit has difficulty in interpreting the corrupted transducer signals because there is spatial and temporal mismatch between the normally
expected and the corrupted signals received.
4. The muscle response pattern generated by the neuromuscular control unit is corrupted, affecting the spatial and temporal coordination and activation of each spinal muscle.
5. The corrupted muscle response pattern leads to corrupted feedback to the control unit via tendon organs of muscles and injured mechanoreceptors (author’s note: and nociceptors), further corrupting the muscle response pattern, (p. 669)
The above stabilization-destabilization scenario is the foundation for why a CSA is clinically indicated for short, intermediate, and long-term treatment (biomechanical stabilization) as clinically indicated. It also clearly outlines that the goal of the CSA is to integrate the bio-neuro-mechanical system to bring the human body to utilize its lowest form of energy for homeostasis, or as close to normal as tissue pathology allows.
This is part of a five-part series, where part one covered the osseous mechanics of what the chiropractic spinal adjustment is comprised of. In part two, we’ve covered the ligamentous involvement from a supportive and neurological perspective. The topic of part three will be spinal biomechanics and its neurological components, and how the chiropractic spinal adjustment makes changes bio-neuro-mechanically. Part four will be an in-depth contemporary comparative analysis of the
chiropractic spinal adjustment versus physical therapy joint mobilization. The final part will be a concise overview of the chiropractic spinal adjustment.
References:
1. Solomonow, M. (2009). Ligaments: A source of musculoskeletal disorders. Journal of Bodywork and Movement Therapies, 13(2),136-154.
2. https://wings, buffalo, edu/eng/mae/courses/417-517/Orthopaedic%20Biomechanics/Lecture%203u.pdf
3. Hauser, R. A., Dolan, E. E, Phillips, H. ./., New I in, A. C., Moore, R. E., & Woldin, B. A. (2013). Ligament injury and healing: A review of current clinical diagnostics and therapeutics. The Open Rehabilitation Journal, 6(1).
4. Solomonow, M. (2006). Sensory-motor control of ligaments and associated neuromuscular disorders. Journal of Electromyography and Kinesiology, 16(6), 549-567.
5. Studin M., Owens W., (2016) Chiropractic spinal adjustments and the effects on the neuroendocrine system and the central nervous system connection. The American Chiropractor, 38(1),46-51.
6. Somatosensory System, The University of Texas, McGovern Medical School, retrieved from: http://neuroscience, uth. tmc. edu/s2/chapter02.html (12/1/20-16).
7. Panjabi, M. M. (2006). A hypothesis of chronic back pain: Ligament subfailure injuries lead to muscle control dysfunction. European Spine Journal, 15(5), 668-676.
Dr. Mark Studin is an adjunct associate professor of chiropractic at the University of Bridgeport College of Chiropractic; an adjunct professor of clinical sciences at Texas Chiropractic College; and a clinical presenter for the State of New York at Buffalo, School of Medicine and Biomedical Sciences for postdoctoral education, teaching MRI spine interpretation, spinal biomechanical engineering, and triaging trauma cases. He also coordinates a clinical rotation in neuroradiology for chiropractic students at the State University of New York at Stony Brook, School of Medicine, Department of Radiology. Dr Studin is also the president of the Academy of Chiropractic teaching doctors of chiropractic how to interface with the medical and legal communities (www.DoctorsPIProgram.com); teaches MRI interpretation and triaging trauma cases to doctors of all disciplines nationally; and studies trends in health care on a national scale (www.TeachDoctors.com). He can be reached at DrMarkfrAcademyojChiropractic.com or at 631-786-4253.
Dr Bill Owens is presently in private practice in Buffalo and Rochester, New York and generates the majority of his new patient referrals directly from the primary care medical community. He is an associate adjunct professor at the State University of New York at Buffalo School of Medicine and Biomedical Sciences as well as the University of Bridgeport, College of Chiropractic, and an adjunct professor of clinical sciences at Texas Chiropractic College. He also works directly with doctors of chiropractic to help them build relationships with medical providers in their community. He can be reached at dr.owensfracademyofchiropractic.com or at 716-228-3847, or by visitingwww.mdreferralprogram.com.