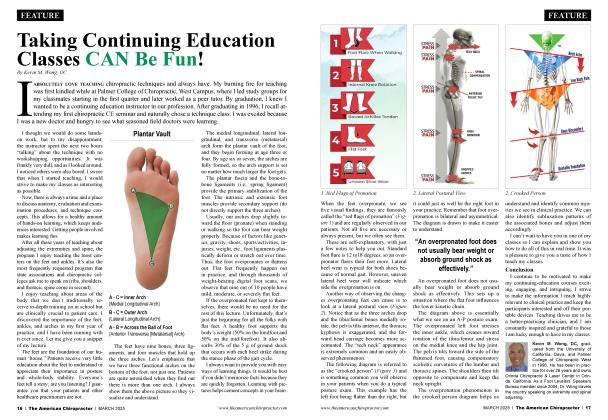
History and Presenting Symptoms A 29-year-old female reports the recent onset of persistent aching pain and tightness in her lower back area. The pain extends into both buttocks, and she occasionally feels it around the right hip and into the right groin. She is into the sixth month of her second pregnancy, and she says that her back pain has increased with her additional weight and postural changes. She reports that she had some back pain during and for a few months after her first pregnancy, but this time it seems much worse. She has been trying to continue with a daily 15-minutc walking program, but is finding tliat difficult because it increases the tension in her lower back region. On a 100 mm visual analog scale (VAS). she rates the pain in her lower back and pehic region as varying from a constant 30 mm to 55 mm recently. Exam Findings Vitals. This expecting female has put on approximately 30 lbs. in the past couple of montlis. and currenth weiglis 178 lbs., which at 5" 7" is within the acceptable range. She has never used tobacco or alcohol. She has had several prenatal checkups and herblood pressure and pulse rate are within normal ranges. Posture and gait. Standing postural evaluation finds a hyper-lordotic lumbar spine and a forward-tilted pelvis, which are associated with her enlarged abdomen. No lateral listing or curvature of her spine is seen, and her iliac crests and greater trochanters are level. She has a slightly widened stance with moderate valgus alignment at the knees. There is also medial bowing of both Achilles tendons, with pes planus and hypcr-pronation bilaterally. During gait, both feet demonstrate an obvious toe-out (foot flare). Chiropractic evaluation. Motion palpation identifies a very tender limitation in scgmcntal motion at the right SI joint, and fixations at L5/S1 and L2/L3. Kemp"s test provokes pain localized to the lower lumbar spine when perfomied to both sides, and reproduces the right hip and groin pain when done to the right. Spinal ranges of motion are otherwise normal and pain-free, and neurologic testing is negative for sensory, motor, and reflexive disorders. Imaging No radiographs were ordered in consideration of her current pregnancy. Clinical Impression Chronic biomechanical strain of the lumbopclvic region exacerbated by postural changes associated with the increased load of pregnancy. There is also poor support from the lower extremities, with excessive pronation interfering with her walking program. Treatment Plan Adjustments. Side posture adjustments were performed to the right sacroiliac joint and the lumbar spinal segments. Support. She was fitted with individually designed stabilizing orthotics based on foot imaging in midstance. The orthotics were designed to provide support for her arches and decrease the biomcchanical stress on her pelvis and sacroiliac joints during her pregnancy and after her delivery. Rehabilitation. She was shown a standing posterior tilt exercise for the pelvis (pelvic extension) to actuate and strengthen the abdominal support muscles and her transverse abdomens in particular. This exercise used the progressive resistance of clastic exercise tubing. She also was instructed to perform abdominal floor exercises (Kcgels). Response to Care The adjustments were well tolerated and resulted in near-immediate release of tension and rapid reduction in pain levels. She adapted easily to her orthotics. and said that she noticed much greater stability in her feet and spine during walking. She performed her daily home exercise program regularly and with no strain or difficulty. She was treated weekly during the remainder of her pregnancy and then for six weeks after her delivery. At that point, she was released to a self-directed maintenance program. Discussion The whole process of pregnancy, delivery, and postpartum places a significant amount of stress on a woman's body. In this case, poor support from the lower extremities increased the biome-chanical strain, resulting in substantial distress. She responded well to the chiropractic adjustments, but she also needed additional support from individually designed stabilizing orthotics and professional guidance for specific postural exercises. (She delivered a healthy 8 lb. 7 oz. baby boy.) Dr. John J. Danchik, the seventh inductee to the AC A Sports Hall ofl'ame, is a clinical professor at Tufts University Medical School and formerly chaired the U.S. Olvmpic Committee's Chiropractic Selection Program. Dr. Danchik lectures on current trends in sports chiropractic and rehabilitation. He can be reached at [email protected] or 617—189-1220.