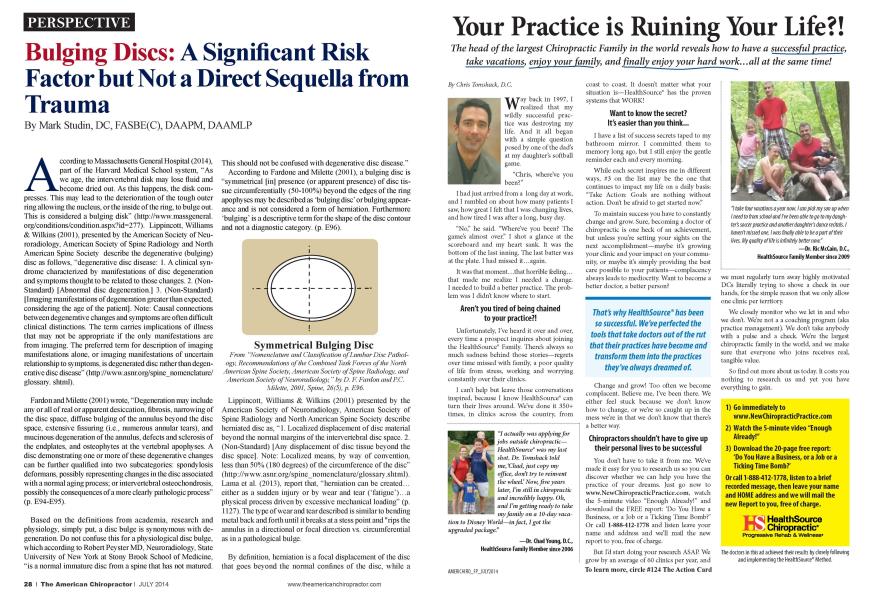
A ccording to Massachusetts General Hospital (2014). part of the Harvard Medical School system. "As we age. the intcn crtcbral disk may lose fluid and become dried out. As this happens, the disk compresses. This may lead to the deterioration of the tough outer ring allowing the nucleus, or the inside of the ring, to bulge out. This is considered a bulging disk" (http://www.massgcncral. org/conditions/condition.aspx?id=277). Lippincott. Williams & Wilkins (2001). presented by the American Society of Ncu-roradiology. American Society of Spine Radiology and North American Spine Society describe the degenerative (bulging) disc as follows, "degenerative disc disease: 1. A clinical syndrome characterized by manifestations of disc degeneration and symptoms thought to be related to those changes. 2. (Non-Standard) |Abnormal disc degeneration.] 3. (Non-Standard) | Imaging manifestations of degeneration greater than expected, considering the age of the patient]. Note: Causal connections between degenerative changes and symptoms are often difficult clinical distinctions. The term carries implications of illness that may not be appropriate if the only manifestations are from imaging. The preferred term for description of imaging manifestations alone, or imaging manifestations of uncertain relationship to symptoms, is degenerated disc rather than degenerative disc disease" (http:/Avww.asnr.org/spinc_nomcnclature/ glossary, shtml). Fardon and Milettc (2001) wrote. "Degeneration may include any or all of real or apparent desiccation, fibrosis. narrowing of the disc space, diffuse bulging of the annulus beyond the disc space, extensive fissuring (i.e.. numerous annular tears), and mucinous degeneration of the annulus. defects and sclerosis of the cndplatcs. and ostcophytcs at the vertebral apophyscs. A disc demonstrating one or more of these degenerative changes can be further qualified into two subcatcgorics: spondylosis deformans. possibly representing changes in the disc associated with a normal aging process: or intcrvcrtcbral ostcochondrosis. possibly the consequences of a more clearly pathologic process" (p. E94-E95). Based on the definitions from academia. research and physiology, simply put. a disc bulge is synonymous with degeneration. Do not confuse this for a physiological disc bulge, which according to Robert Pcystcr MD. Neuroradiology. State University of New York at Stony Brook School of Medicine, "is a normal immature disc from a spine that has not matured. This should not be confused with degenerative disc disease."" According to Fardonc and Milettc (2001). a bulging disc is "symmetrical [in] presence (or apparent presence) of disc tissue circumfcrcntially (50-100%) beyond the edges of the ring apopln ses may be described as 'bulging disc" or bulging appearance and is not considered a form of hcrniation. Furthermore "bulging" is a descriptive term for the shape of the disc contour and not a diagnostic category, (p. E96). Symmetrical Bulging Disc I'mm "Xomenclatuiv and (Classification of Lumbar Disc Pathology, Recommendations of the Combined Task Vorces of the Xorth American Spine Society, American Society of Spine Radiology, and American Society ofXeummdiology, " bv D. /'.' Fanlon and P.C. Milette, 2001, Spine, 26(5), p. E96. Lippincott. Williams & Wilkins (2001) presented by the American Society of Neuroradiology. American Society of Spine Radiology and North American Spine Society describe hcrniated disc as. "1. Localized displacement of disc material beyond the normal margins of the inten ertebral disc space. 2. (Non-Standard) [Any displacement of disc tissue beyond the disc space]. Note: Localized means, by way of convention, less than 50% (180 degrees) of the circumference of the disc" (http:/Av\v\v.asnr.org/spine_nomenclature/glossary.shtml). Lama et al. (2013). report that, "herniation can be created... either as a sudden injury or by wear and tear ("fatigue")...a physical process driven by excessive mechanical loading" (p. 1127). The type of wear and tear described is similar to bending metal back and forth until it breaks at a stess point and "rips the annulus in a directional or focal direction vs. circumferential as in a pathological bulge. By definition, herniation is a focal displacement of the disc that goes beyond the normal confines of the disc, while a bulge is a circumferential displacement of the disc material that although by definition covers 50-100% of the circumference, usually covers close to 100% of the disc. To explain this colloquially, it's like pushing on an Oreo cookie: the cream pushes out evenly around the entire disc-shaped cookie or circumferentially. Clinically, the type of bulges seen in post-trauma patients are degenerative bulges, with physiologic bulges reserved to those immature discs in pre-pubescents. These are differentiated from hcrniations simply based upon the morphology (appearance) of the disc and in conjunction with a detailed history, needs to be clinically correlated to the causal relationship to conclude an accurate diagnosis. With aging, you will have both disc and cndplatc degeneration and according to Fardone and Milctte (2001). "...affects essentially the annulus fibrosis and the adjacent apophyscs..." (p. E99). This process takes montlis. even years to develop and cannot be directly correlated to a trauma that occurred a few days, weeks or months just prior to the acquiring of the MRI image. There simply isn't enough time for the degeneration to occur. CLINICAL PRACTICE NOTE: If your patient has a diagnosis of a bulged disc and the MRI was taken within 3-4 months of the trauma that diagnosis is not as Scquclla from the recent trauma. Disc bulges can be directly from trauma if the image and resultant diagnosis is acquired approximately 1 year post-trauma where the disc has time to degenerate from the trauma-related pathology. This is typically found by surgeons who arc considering invasive care, where the doctor focusing on spinal correction and/or rehabilitation typically orders the images cither immediately or within a few montlis of the trauma based upon clinical presentation. BULGING DISC AS A RISK FACTOR According to Garcia-Cosamalon et al. (2010). "nerve fibers in the intcrvcrtcbral discs are found mostly in the periphery of the annulus fibrosis. The sensory fibers that innervate the intcrvcrtcbral disc are mainly nociceptive and. to a lesser extent, proprioceptivc" (page 1). "In the degenerated IVD [intcrvcrtcbral discs], nerve fibers are increased in number and they enter the inner layers of the AF [annulus fibrosis | and even the nucleus pulposus (NP). Furthermore, in these conditions, the density of mechanoreccptors in the superficial layers of the IVDs lintervcrtcbral discs] is increased"" (Garcia-Cosamalonct al.. 2010. p. 4. Fig. 2). Nonnal Intcrvcrtcbral Disc Xon-peptodergic small sized neurons Ret/ * GFRA1. Gl-Ra3IB4 VR1. P2X3 TMP • Peptodergic small sized neurons/ TrkA+/TrkB/GFRa3/CGRP/SP/TRPY 1 | Intermediate sized neurons/Trk8/ Ret/GFRa3/CGRP/SP TRPV1 Large sized ncurons/Trk C+/Ca2-binding proteins/liNaCs TRP ion Degenerated Intervertebral Disc From "Inlerverlebral Disc, Sensory Nerves and Xeumtmphin.s: Who is Who in Discogenic Pain?, "byJ. Garcia-C osamalon, A/. /:'. del lalle, M. G. Calavia, O. Garcia- This indicates that bulging discs have nerves that arc "ingrown" into the inner annulus and nucleus and are risk factors for the trauma case where you now have innervations that are more sensitive in nature due to the new growth. Therefore, an initialing factor of trauma will potentially cause more pain with less force in the degenerated or bulged disc. CLINICAL NOTE: In the presence of a bulging disc and an absence of cord or root compression or thecal sac involvement (which, too. has A. B and C sensory fibers in the arachnoid layer of the thecal sac), the bulge becomes the competent producing factor for the discogenic pain of your patient. As a result, it would indicate that adjustments specifically at these levels be avoided and correction and stabilization of the spine should occur above and below the level of lesion. CONCLUSION: Pathological disc bulges are degenera- the in etiology in the post-pubescent patient and arc not directly caused from trauma. These patients, as a result of the risk factor of a disc bulge and as evidenced by an MRI that either meets or exceeds, as reported by Studin (2013), the Guidelines of the American College of Radiology for acquisition of slice thicknesses and sequence protocols will be susceptible to greater pain as sequella with less force. The pain has also been clinically evidenced to persist upwards for the lifetime of the patient. With this category of patient, the clinician should consider treating and stabilizing the adjacent regions of the spine and supportive connective tissues. Typically, this patient has a poorer prognosis that will consistently de-stabilize and require more frequent care as a result of the degeneration and pain generators. Refetvnces: 1 .MassadmsettsGenemll laspital (2014). Liimbardiscdisease.Condi-tiav>&'Hvatmenls,RelriewdXin'21,201-IJioniliIlp: -wwwmassgeneml. otg conditions condition.aspx?id 277 2.Lippincotl, Williams & H'illdn.s(2001). Xonienckitwv and classificci-tioiiqPimibarctx'pcidiology;GIosx»y..-lniericaiJainialofXetin)nuSol-ogy; Ret>ie\>edMay>21, 2014,fivmhttp://www.asnr.o>%'spine ncniencla-twv glassaiy.slitnil h'ardon, 11 /'.', &\ lilette, P.C. (2001). Nomenclativeand'classification qftxmilxnxUscpatlmk^Reccmmkmihtioiisoftiieconibiiiedtaskfoirxscf the Xouli .Inierican Spine Society; American Society of Spine Radiology; and.lmerican Society of Xewotrtdiology. Spine, 26(5), H93-H113. Umia, R. Ix'.\/aitie C. L. Dokm, P., Tariton, J. K. Haniing, 1.1. & Adams, M.A. (2013). Do intervertebraldiscs degenerate before they hemiate, or- after? Ihe Bate & Joint Journal, 95-B(8), 1127-1133. 5. Garcia-Cosarrtalon,./., del I idle, M. /;., Ca-Icn'ia, M. G., Gmaa-Suarvz, ()., Ix>pez-\ luniz. A., Otem.J., & lega.J.A. (2010). Iitterveitebnddisc, sensory nerves aid newotrvphins: Who is who in discojienic pain? Journal of'.- bicttonw, 217(1), 1-15. S.Sntdin.M. (2013). livatingpatientswitlulisc heniialions. Pan 1 :.\ till ordering protocols. Ihe American (liiropractor; 35(11), 28,30,32-33. Dr. Mark Studin is an adjunct assistant professor in clinical sciences at the I niversity of Bridgeport College of Chiropractic and a clinical presenter for the State of New York at Buffalo, School of Medicine and Riomedical Sciences for post-doctoral education, teaching MRI spine interpretation and triaging trauma cases. He is also the president of the Academy of Chiropractic teaching doctors of chiropractic how to interface with the legal community (www.Law-yersPlProgram.com) and teaches MRI interpretation and triaging trauma cases to doctors of all disciplines nationally (www.TeachDoctors.com). He can be reached at DrMark'xlTeachDoctors. com or at 631-786-4253.