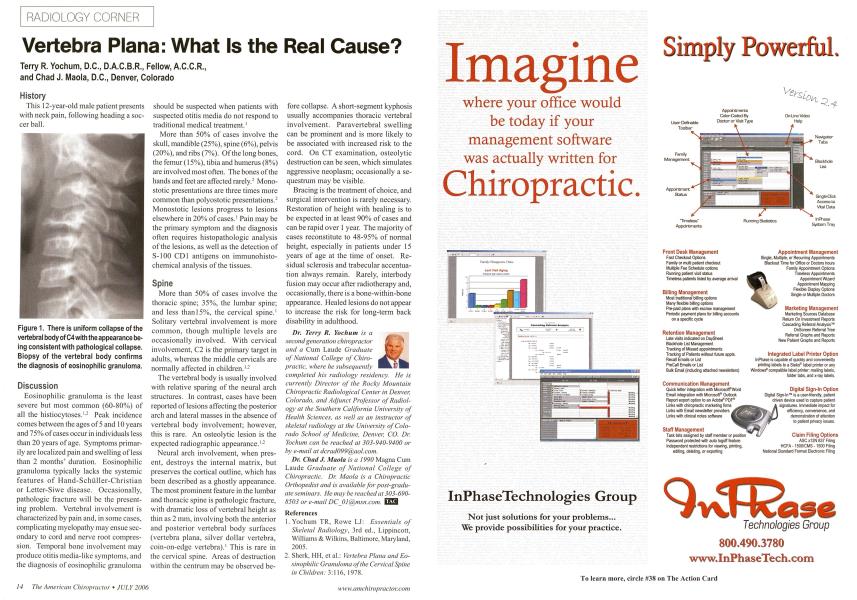
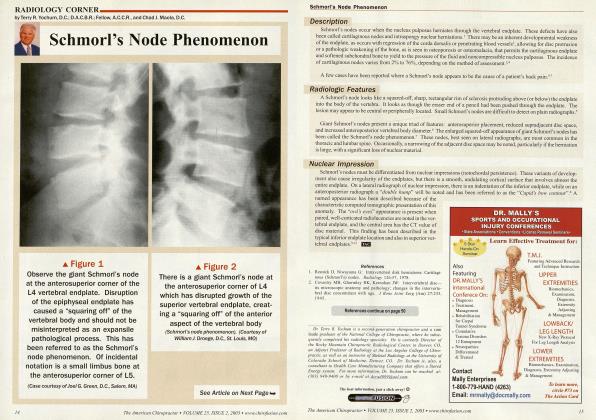
History This 12-year-old male patient presents with neck pain, following heading a soccer ball. Discussion Eosinophilic granuloma is the least severe but most common (60-80%) of all the histiocytoses.12 Peak incidence comes between the ages of 5 and 10 years and 75% of cases occur in individuals less than 20 years of age. Symptoms primarily are localized pain and swelling of less than 2 months' duration. Eosinophilic granuloma typically lacks the systemic features of Hand-Schiiller-Christian or Letter-Siwe disease. Occasionally, pathologic fracture will be the presenting problem. Vertebral involvement is characterized by pain and, in some cases, complicating myclopathy may ensue secondary to cord and nerve root compression. Temporal bone involvement may produce otitis media-like symptoms, and the diagnosis of eosinophilic granuloma should be suspected when patients with suspected otitis media do not respond to traditional medical treatment.1 More than 50% of cases involve the skull, mandible (25%), spine (6%), pelvis (20%), and ribs (7%). Of the long bones, the femur (15%), tibia and humerus (8%) are involved most often. The bones of the hands and feet are affected rarely.2 Mono-stotic presentations are three times more common than polyostotic presentations.: Monostotic lesions progress to lesions elsewhere in 20% of cases.1 Pain may be the primary symptom and the diagnosis often requires histopathologic analysis of the lesions, as well as the detection of S-100 CD1 antigens on immunohisto-chemical analysis of the tissues. Spine More than 50% of cases involve the thoracic spine; 35%, the lumbar spine; and less than 15%, the cervical spine.1 Solitary vertebral involvement is more common, though multiple levels are occasionally involved. With cervical involvement, C2 is the primary target in adults, whereas the middle cervicals are normally affected in children.12 The vertebral body is usually involved with relative sparing of the neural arch structures. In contrast, cases have been reported of lesions affecting the posterior arch and lateral masses in the absence of vertebral body involvement; however, this is rare. An osteolytic lesion is the expected radiographic appearance.1-2 Neural arch involvement, when present, destroys the internal matrix, but preserves the cortical outline, which has been described as a ghostly appearance. The most prominent feature in the lumbar and thoracic spine is pathologic fracture, with dramatic loss of vertebral height as thin as 2 mm, involving both the anterior and posterior vertebral body surfaces (vertebra plana, silver dollar vertebra, coin-on-edge vertebra).1 This is rare in the cervical spine. Areas of destruction within the centrum may be observed be- fore collapse. A short-segment kyphosis usually accompanies thoracic vertebral involvement. Paravertebral swelling can be prominent and is more likely to be associated with increased risk to the cord. On CT examination, osteolytic destruction can be seen, which simulates aggressive neoplasm; occasionally a sequestrum may be visible. Bracing is the treatment of choice, and surgical intervention is rarely necessary. Restoration of height with healing is to be expected in at least 90% of cases and can be rapid over 1 year. The majority of cases reconstitute to 48-95% of normal height, especially in patients under 15 years of age at the time of onset. Residual sclerosis and trabecular accentuation always remain. Rarely, interbody fusion may occur after radiotherapy and, occasionally, there is a bone-within-bone appearance. Healed lesions do not appear to increase the risk for long-term back disability in adulthood. Dr. Terry R. Yoclium is a second generation chiropractor and a Cum Laude Graduate of National College of Chiropractic, where he subsequently completed his radiology residency. He is currently Director of the Rockv Mountain Chiropractic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology at the Southern California University of Health Sciences, as well as an instructor of skeletal radiology at the University of Colorado School of Medicine, Denver, CO. Dr. Yoclwm can be reached at 303-940-9400 or by e-mail at [email protected]. Dr. Chad J. Maola is a 1990 Magna Cum Laude Graduate of National College of Chiropractic. Dr. Maola is a Chiropractic Orthopedist and is available for post-graduate seminars. He may be reached at 303-690-8503 or e-mail DCOKw.msn.com. EZS References Yochum TR, Rovve LJ: Essentials of Skeletal Radiology, 3rd ed., Lippincott, Williams & Wilkins, Baltimore, Maryland, 2005. Sherk, HH, ct al.: Vertebra Plana and Eo- sinophilic Granuloma of the Cervical Spine in Children: 3:116. 1978. Figure 1. There is uniform collapse of the vertebral body of C4 with the appearance being consistent with pathological collapse. Biopsy of the vertebral body confirms the diagnosis of eosinophilic granuloma.