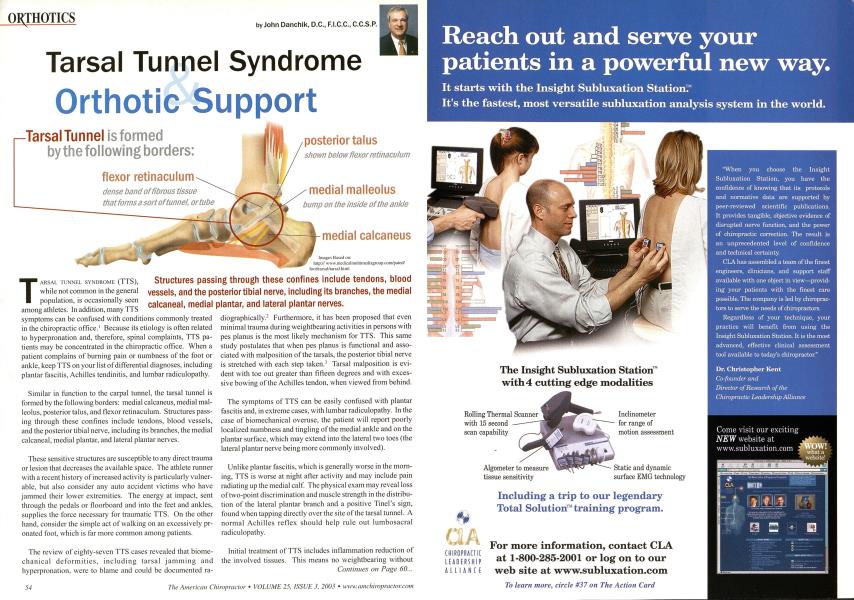
T ARSAL TUNNEL SYNDROME (TTS), while not common in the general population, is occasionally seen among athletes. In addition, many TTS symptoms can be confused with conditions commonly treated in the chiropractic office.' Because its etiology is often related to hyperpronation and, therefore, spinal complaints, TTS patients may be concentrated in the chiropractic office. When a patient complains of burning pain or numbness of the foot or ankle, keep TTS on your list of differential diagnoses, including plantar fascitis, Achilles tendinitis, and lumbar radiculopathy. Similar in function to the carpal tunnel, the tarsal tunnel is formed by the following borders: medial calcaneus, medial mal-leolus, posterior talus, and flexor retinaculum. Structures passing through these confines include tendons, blood vessels, and the posterior tibial nerve, including its branches, the medial calcaneal, medial plantar, and lateral plantar nerves. These sensitive structures are susceptible to any direct trauma or lesion that decreases the available space. The athlete runner with a recent history of increased activity is particularly vulnerable, but also consider any auto accident victims who have jammed their lower extremities. The energy at impact, sent through the pedals or floorboard and into the feet and ankles, supplies the force necessary for traumatic TTS. On the other hand, consider the simple act of walking on an excessively pr-onated foot, which is far more common among patients. The review of eighty-seven TTS cases revealed that biome-chanical deformities, including tarsal jamming and hyperpronation, were to blame and could be documented ra- diographically.2 Furthermore, it has been proposed that even minimal trauma during weightbearing activities in persons with pes planus is the most likely mechanism for TTS. This same study postulates that when pes planus is functional and associated with malposition of the tarsals, the posterior tibial nerve is stretched with each step taken.' Tarsal malposition is evident with toe out greater than fifteen degrees and with excessive bowing of the Achilles tendon, when viewed from behind. The symptoms of TTS can be easily confused with plantar fascitis and, in extreme cases, with lumbar radiculopathy. In the case of biomechanical overuse, the patient will report poorly localized numbness and tingling of the medial ankle and on the plantar surface, which may extend into the lateral two toes (the lateral plantar nerve being more commonly involved). Unlike plantar fascitis, which is generally worse in the morning, TTS is worse at night after activity and may include pain radiating up the medial calf. The physical exam may reveal loss of two-point discrimination and muscle strength in the distribution of the lateral plantar branch and a positive Tinel's sign, found when tapping directly over the site of the tarsal tunnel. A normal Achilles reflex should help rule out lumbosacral radiculopathy. Initial treatment of TTS includes inflammation reduction of the involved tissues. This means no weightbearing without Continues on Page 60... ...From page 54 the foot and ankle taped or without orthotics in place. Next, adjustments should be used to restore normal biomechanics throughout the entire kinetic chain (foot, ankle, knee, hip, and spine). Special attention must be given to the valgus misalignments of the talus and calcaneus. Additionally, deep friction massage over the flexor retinaculum may release adhesions responsible for compression symptoms. Most importantly, correct the underlying foot dysfunction (hyperpronation or otherwise). Pes planus causes tightening of the flexor retinaculum, which can then compress structures within the tunnel. Although the inflammation may go away, the nature of ligament stretch means that any plastic deformation is permanent (barring surgical intervention). Therefore, effective and lasting treatment necessitates the use of custom-made, flexible orthotics, which have been demonstrated to control the degree of pronation, as well as the percent of time spent in pronation. Although relatively uncommon, tarsal tunnel syndrome can present a diagnostic and treatment challenge. Understanding the etiology of this entrapment syndrome is important for providers concerned with the treatment of athletes and auto-accident victims. Also, because TTS is often associated with hyperpronation, patients will likely experience other conditions also associated with a faulty foundation, including knee, hip, and low back pain. Many of these patients will seek care from chiropractors, where treatment consisting of adjustment, soft-tissue technique, and the use of flexible orthotics can offer excellent symptom relief. See page 59 for References Dr. John J. Danchik is the seventh inductee to the American Chiropractic Association Spoils Hall of Fame. He is the current Tarsal Tunnel Syndrome Close-Up i Structures passing through these confines include tendons, blood vessels, and the posterior tibial nerve, including its branches, the medial calcaneal, medial plantar, and lateral plantar nerves. As the pressure increases in the tarsal tunnel, the nerve is the most sensitive to the pressure and is squeezed against the flexor retinaculum. Special attention must be given to the valgus misalignments of the talus and calcaneus.