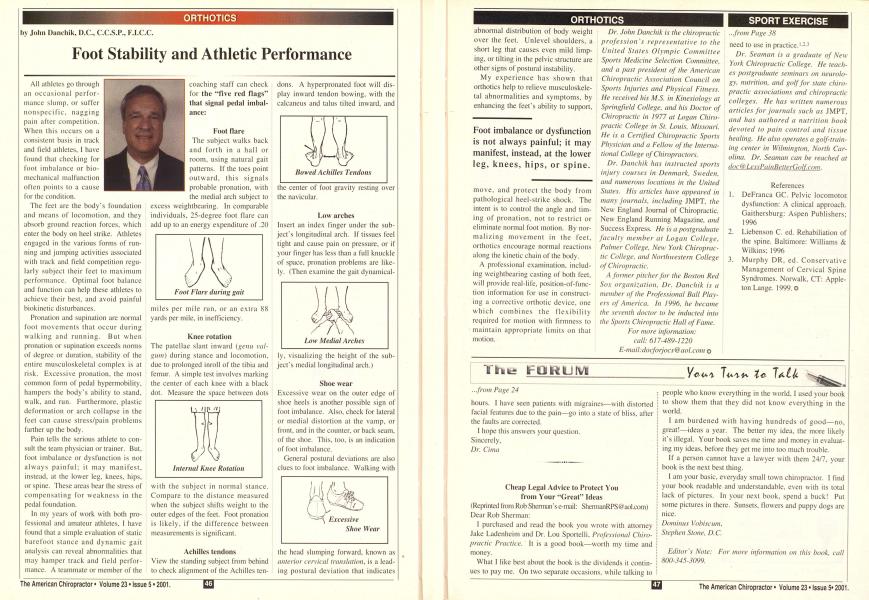
All athletes go through an occasional performance slump, or suffer nonspecific, nagging pain after competition. When this occurs on a consistent basis in track and field athletes, I have found that checking for foot imbalance or bio-mechanical malfunction often points to a cause for the condition. The feet are the body's foundation and means of locomotion, and they absorb ground reaction Ibices, which enter the body on heel strike. Athletes engaged in the various forms of running and jumping activities associated with track and field competition regularly subject their feet to maximum performance. Optimal foot balance and function can help these athletes to achieve their best, and avoid painful biokinetic disturbances. Pronation and supination are normal foot movements that occur during walking and running. But when pronation or supination exceeds norms of degree or duration, stability of the entire musculoskeletal complex is at risk. Excessive pronation. the most common form of pedal hypermobility. hampers the body's ability to stand, walk, and run. Furthermore, plastic deformation or arch collapse in the feet can cause stress/pain problems farther up the body. Pain tells the serious athlete to consult the team physician or trainer. But. foot imbalance or dysfunction is not always painful; it may manifest, instead, at the lower leg. knees, hips, or spine. These areas bear the stress of compensating for weakness in the pedal foundation. In my years of work with both professional and amateur athletes. I have found that a simple evaluation of static barefoot stance and dynamic gait analysis can reveal abnormalities that may hamper track and field performance. A teammate or member of the coaching staff can check for the "five red flags" that signal pedal imbalance: Foot flare The subject walks back and forth in a hall or room, using natural gait patterns. If the toes point outward, this signals probable pronation, with the medial arch subject to excess weightbearing. In comparable individuals. 25-degree foot flare can add up to an energy expenditure of .20 miles per mile run. or an extra 88 yards per mile, in inefficiency. Knee rotation The patellae skint inward (f>cnn val-guin) during stance and locomotion, due to prolonged inroll of the tibia and femur. A simple test involves marking the center of each knee with a black dot. Measure the space between dots with the subject in normal stance. Compare to the distance measured when the subject shifts weight to the outer edges of the feet. Foot pronation is likely, if the difference between measurements is significant. Achilles tendons View the standing subject from behind to check alignment of the Achilles ten- dons. A liyperpronated foot will display inward tendon bowing, with the calcaneus and talus tilted inward, and the center of foot gravity resting over the navicular. Low arches Insert an index finger under the subject's longitudinal arch. If tissues feel tight and cause pain on pressure, or if your finger has less than a full knuckle of space, pronation problems arc likely. (Then examine the gait dynamical- ly, visualizing the height of the subject's medial longitudinal arch.) Shoe wear Excessive wear on the outer edge of shoe heels is another possible sign of foot imbalance. Also, check for lateral or medial distortion at the vamp, or front, and in the counter, or back seam, of the shoe. This, too, is an indication of foot imbalance. General postural deviations are also clues to foot imbalance. Walking with the head slumping forward, known as anterior cervical translation, is a leading postural deviation that indicates abnormal distribution of body weight over the feet. Unlevel shoulders, a short leg that causes even mild limping, or tilting in the pelvic structure are other signs of postural instability. My experience has shown that oithotics help to relieve musculoskele-tul abnormalities and symptoms, by enhancing the feet's ability to support. move, and protect the body from pathological heel-strike shock. The intent is to control the angle and timing of pronation. not to restrict or eliminate normal foot motion. By normalizing movement in the feet. orthotics encourage normal reactions along the kinetic chain of the body. A professional examination, including weightbearing casting of both feet, will provide real-life, position-of-func-tion information for use in constructing a corrective orthotic device, one which combines the flexibility required for motion with firmness to maintain appropriate limits on that motion. Dr. John Danchik is the chiropractic profession 's representative to the United States Olympic Committee Sports Medicine Selection Committee, and a past president of the American Chiropractic Association Council on Sports Injuries and Physical Fitness. He received his M.S. in Kinesiology at Springfield College, and his Doctor of Chiropractic in 1977 at Logan Chiropractic College in St. Louis, Missouri. He is a Certified Chiropractic Sports Physician and a Fellow of the International College of Chiropractors. Dr. Danchik has instructed sports injury courses in Denmark, Sweden, and numerous locations in the United States. His articles have appeared in many journals, including JMPT. the New England Journal of Chiropractic, New England Running Magazine, and Success Express. He is a postgraduate faculty member at Logan College, Palmer College, New York Chiropractic College, and Northwestern College of Chiropractic. A former pitcher for the Boston Red Sox organization. Dr. Danchik is a member of the Professional Ball Players of America. In 1996, he became the seventh doctor to be inducted into the Sports Chiropractic Hall of Fame. For more information: call: 617-4X9-1220 E-mail:docforjocs @ aol. com o