Eliminate Eliminators
By Eric Kaplan DC, FIAMA, Perry Bard, DC & Jason Kaplan, DC
Doctors, I want to ask you a question today. What percentage of your patients follow through with their treatment program? What percentage of your patients refer others? Dr. Bard and I have found that patients discontinue care because it’s hard to understand 100% of what we do from a 15-minute report of findings. Education is an ongoing process to eliminate eliminators, i.e., it is your responsibility to prepare the staff for questions that patients may report.
Disc Centers of America (DCOA) now has over 230 clinics in 45 states, and doctors always ask about our secret to success. We simply try to make our doctors better physicians, not salespeople, to eliminate eliminators. To do that, provide patients with research that justifies your treatment program because it makes your presentation seem more objective than subjective. We bombard our clients with medical research justifying the utilization and necessity of nonsurgical spinal decompression (NSSD).
Use excuse eliminators to get past common reasons patients will give for not following through with regular appointments or discontinuing care prematurely. Make the patient think about their commitment to receive proper care. By asking questions, you can force them to see their excuse. When used properly, the only reason a patient will quit is if a genuine problem exists, which can occur in a few cases. Excuses from the patient should be followed with a question pertaining to their excuse.
One of my favorite studies is the Leslie study (found at Thebestdiscbook.com), which observed improvement over a six-week period. Study after study shows the necessity of spinal decompression ranging from a 17-visit protocol from Dr. Yokum to a 40-visit treatment plan by neuroradiologist Dr. Eyerman.
Our report of findings eventually ends with an agreement. I tell all my patients if they miss 50% of the appointments, they can only expect 50% of the results. In this article, I want to give you valuable tips, scripts, and questions that you or your staff can ask patients.
You can remind patients that they have agreed to a course of care by saying any of the following suggestions during a visit:
1. What makes you think it’s safe to quit coming?
3. Where did you get the idea that “being so busy” corrected your problem all of a sudden?
5. Tell me what is so much more important than your health.
7. Did the doctor say you would be well this soon, or did he say it would take at least 90 days?
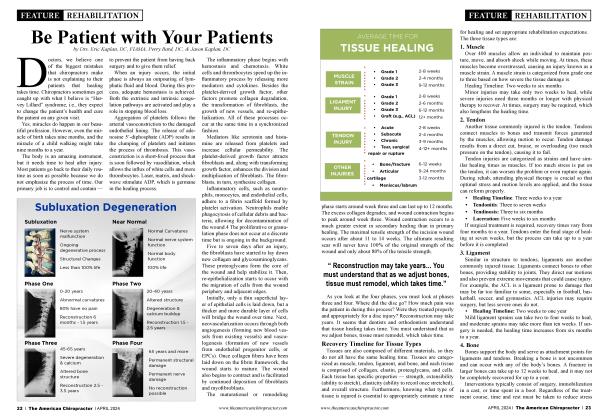
9. When joints move, the ligaments stay flexible; when they don’t, the ligaments get stiff, and deterioration is inevitable.
11. Drugs and surgery can patch up the pain but will not restore mobility. Sooner or later, you’ll have to get this taken care of properly.
13. Feeling better? That’s great! Now we can focus on corrective spine care to minimize the amount of permanent residual damage.
15. If you were a member of the doctor’s family, he would recommend the same thing. In fact, he did tell his (mother/father/sibling/etc.) this. (Use only when this is true!)
17. We’re not just treating you for what you have now. We’re treating you for what you will have if this isn’t taken care of properly.
19. Of course, you’ll never be totally free from any form of treatment; you’re never free from dental care either. Don’t you brush your teeth every day? Our goal is to get you as well as we can as soon as possible, teach you how to take care of your spine, and check on you periodically to make sure your spine is moving and as free as possible from serious consequences.
21. Consistency is very important. With all that scar tissue, your ligaments will resist movement until they are retrained and become more elastic. You will lose ground if you miss appointments, and it will take more adjustments to reach our goal.
23. Restricted motion due to injury, lack of use, or both will result in joint deterioration. The only way to see any real results is to restore the motion and keep it moving.
25. Didn’t you say you wanted your condition controlled and stabilized rather than just patch it up with minimum care? Fine, let’s get back on the program.
27. Remember what those nerves looked like on the chart? How would you like that worn-out nerve going to your leg/arm/stomach/prostate/uterus/etc.? (We love Visual Odyssey by Bruce Goldsmith, if you have that program.)
29. If we can’t help you, we will tell you.
31. We have medical, orthopedic, neurological, chiropractic, MRI, and X-ray tests, and they all verify each other.
33. What did the other doctor say about those compressed vertebrae?
35. As long as your spine remains in its present state, you are guaranteed to have degeneration and pinched nerves. Is that what you want?
37. You need to maintain the mobility we achieved in your spine because there is residual damage, and your problem will return. Don’t you want to keep your spine mobile so it will have a fighting chance?
In closing, an office visit has six essential components, each of which must be performed to treat the patient properly and maintain patient control.
Ask the patient how they are progressing.
We have been told not to ask the patient about their condition because it engages the doctor in conversation and slows them down. That is a major mistake. You should ask every patient how they are progressing. It improves the doctor/patient relationship, reduces malpractice risk, and helps speed the patient’s healing.
However, wait to ask the patient how they are progressing until you have positioned them so that you can work with them while the patient is responding. For instance, ask the patient how they are doing while using laser, shockwave, or an adjustment instrument. The Accu-SPINA decompression table will not commence unless you put in a pain number. Ongoing Oswestry tests are also good.
Tell the patient how they appear.
Never ask patients how they are progressing without immediately telling them how they appear to be doing. After the patient responds to your question about their progress, you should follow their response with a statement about how they appear. For example, you might say, “I am glad to hear you haven’t had any headaches for the last two weeks. I do notice when I run this instrument on your back that you still have some heat-sensitive areas, and your neck doesn’t move through its full range of motion as well as it should yet. I am glad you’re getting better, but we’ll need to keep working on that area.”
Grade your treatment/adjustment.
You should grade each visit. By grading your adjustment, you show the patient that you are happy with your results and their progress. I’ve written a past article about how healing takes time. Nature moves at its own pace. You can be a great doctor, but every patient has their own innate healing abilities. Whether a positive minor sign or a brief test of range of motion, make a quick evaluation of patients during each revisit.
Example 1: That’s the best treatment we’ve gotten this week.
Example 2: That’s exactly what I wanted.
Example 3: That treatment seems to set better almost every time.
Offer encouragement.
One of the best procedures for keeping patients under care is constantly encouraging their progress. Simply say something such as, “You’re progressing just like I anticipated. That’s encouraging.” The key is always being honest and keeping the patient involved in their care.
Confirm the next appointment.
I started this habit early on in my practice. After you have completed the treatment, be sure to firm up the next appointment with the patient. If the missed appointment percentage in your office is 10% or less, firming up an appointment can be very casual. “I’ll see you on your next visit.” However, if your missed appointment percentage is above 10%, be sure to firm up the appointment and request confirmation from the patient.
Mention maintenance
This is the most difficult step in the six-point office visit because it is not done during each visit, so it is the most difficult to implement. Concierge Coaches suggests that you discuss maintenance with patients during four specific visits:
When the patient first sees definite relief (usually between the 12 and 20 visits).
After the patient has seen total or near total symptomatic relief (usually near the end of care).
During the re-report, which is given on the last visit. I recommend giving the patient exercises and doing a reevaluation and re-report two weeks after the commencement of rehabilitative exercise.
After they return from their two-week layoff, examine, reevaluate, and maybe even X-ray again to view their structural subluxation complex, symptoms, and disc space.
Using this six-point procedure for every patient visit increases your chance of patient compliance and practice growth immeasurably. This article is about education and reeducation. Don’t be so naïve or arrogant to believe that you can do one report of findings and that the patient will totally understand what you do and what took you years to learn.
Dr. Eric Kaplan and Dr. Perry Bard, are business partners of over 32 years. They have developed Disc Centers of America & Concierge Coaches. Currently, they have over 150 clinics using their Disc Centers of America brand and lead ongoing success training events throughout the year. For more information on coaching, spinal decompression, or seminars, visit www.thechiroevent.com or www.decompressioncertified.org, or call the Chiropractic Q&A Hotline at 888-990-9660.
Dr. Jason Kaplan is a graduate of Parker University. Along with his wife Dr. Stephanie Kaplan, they practice in Wellington Florida. Jason is an Instructor for Disc Centers of America, one of the Nation’s largest collection of doctors specializing in Disc Injuries. He has been recognized and honored by the International Disc Education Association and teaches technique at the National Certification Program at Life University and is considered a Master on Non Surgical Spinal Decompression, www.wellingtondisccenter.com.