An AK Approach to the Krebs Cycle
BIOCHEMISTRY
Dysfunction and Beyond
Richard Belli
DC, DACNB, FABNN
We need ATP not just for physical exercise but for every biochemical reaction that takes place in the body. At the heart of the cell is a merrygo-round of energy and matter known as the Krebs cycle. It is also sometimes called the “citric acid cycle” or the “tricarboxylic acid cycle,” but for this discourse, we will stick with the common name of the Krebs cycle.
Each step in the Krebs cycle is an ostensibly trivial rearranging of carbon, hydrogen, and oxygen atoms with a byproduct of carbon dioxide. Textbooks tell us that the Krebs cycle generates energy by stripping out hydrogen atoms from the carbon skeletons of food and feeding them to the ravenous beast that is oxygen, which is the process of cellular respiration. The energy released at each step is ingeniously captured and used in the cell, while the inert carcass of water and carbon dioxide is discharged to the outside world.
You will read that the Krebs cycle is about the oxidation of foodstuffs, and especially glucose to synthesize ATP. In addition to the primary source of ATP, the Krebs cycle is considered the engine of biosynthesis. For example, most amino acids are directly or indirectly from molecules in the Krebs cycle, as are the long-chain lipid molecules needed to make cell membranes. Even the letters of DNA termed nucleotides are made from sugars and amino acids also derived from the Krebs cycle.
The Krebs cycle is also important for production of neurotransmitters, including the excitatory neurotransmitter glutamate and the inhibitory neurotransmitter GABA. Glutamate is directly produced by the Krebs cycle, then converted to GABA via a decarboxylation reaction and a cofactor peridoxal-5-phosphate, the phosphorylated form of B6. The balance of glutamate and GABA production is imperative for normal cerebral cortex function. This imbalance can lead to disorders of mood, anxiety, and in extreme cases, seizures.
Considering the previous discussion, it is very easy to appreciate the myriad of symptoms and maladies that may occur with dysfunction of the Krebs cycle, including everything from fatigue, pain, digestive disorders, anxiety, and heart issues.
Krebs cycle dysfunction is so impotent that it is hard to believe a patient can move toward optimal health until it is corrected. Therefore, two questions immediately come to mind: what causes Krebs cycle dysfunction, and how do we treat it?
The Krebs cycle is susceptible to many assaults, which include a simple lack of vitamin and mineral cofactors, toxins, virus, inflammatory hormones, immune cytokines, alcohol, heavy metals, and other commonly abused substances.
Before we can fix the Krebs cycle, we need to have a clinical predictor of dysfunction. Referring to our early discussion, you will remember that a byproduct of ATP production is carbon dioxide. Carbon dioxide is not a waste product, as many would think. It is used for many important reactions in the body, including respiration, kidney function, and hydrochloric acid and pancreatic acid production, to mention a few. Therefore, if the mitochondria are not producing enough carbon dioxide, metabolic dysfunctions will likely occur.
We can easily identify Krebs cycle dysfunction with manual muscle testing and increasing carbon dioxide (Co2). Simply identify an inhibited or weak muscle and have the patient rebreathe their own air to increase Co2 titers. Rebreathing is simply done using a brown paper lunch bag. The patient covers both the nose and mouth with the bag and rebreathes six to eight breaths. If rebreathing facilitates the inhibited muscle, one can assume that there is a decrease in Co2 titers because of Krebs cycle dysfunction.
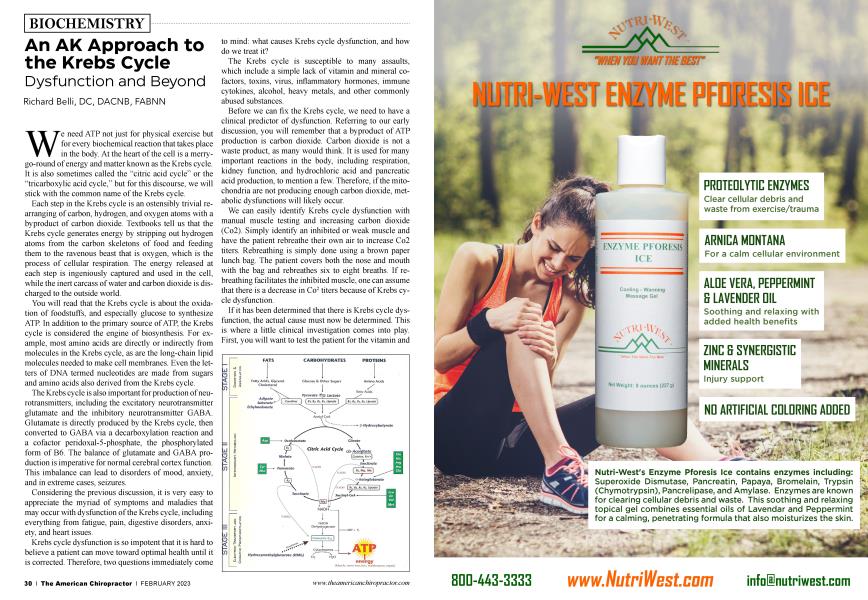
If it has been determined that there is Krebs cycle dysfunction, the actual cause must now be determined. This is where a little clinical investigation comes into play. First, you will want to test the patient for the vitamin and mineral cofactors that make the Krebs cycle spin. These include Bl, B2, B3, B5, lipoic acid, manganese, and magnesium, as indicated below.
Additionally, coenzyme Q10 is necessary for the final step in ATP production called the electron transport chain. Coenzyme Q10 is depleted by medications, including statins. Also, phosphorylated B6 or P-5-P is necessary for Q10 synthesis in the liver. One or more of the above may strengthen the inhibited muscle, which indicates a need for supplementation.
Once ATP cofactors have been examined and necessity determined, it will be wise to address the other Krebs cycle inhibitors that were previously mentioned, including free radical damage from insufficient antioxidants and insufficient subcellular melatonin from lack of exposure to near infrared sun rays.
Taking it beyond the Krebs cycle, we can see that it is necessary to look at the effects of ATP production and other byproducts, such as glutamate, GABA, and adenosine.
Adenosine is essential for proper function of every cell in the body. It is important to know that ATP acts as an excitatory co-transmitter, with norepinephrine and adenosine as an inhibitory neurotransmitter. ATP gets metabolized to adenosine with a hydrolysis reaction and magnesium as a cofactor. When awake, adenosine rises by the hour, resulting in the desire to sleep or sleep pressure. If Krebs cycle dysfunction is corrected and the patient becomes more irritable or doesn’t feel like sleeping, magnesium supplementation may be necessary to move from ADP to adenosine, as indicated below. And finally, adenosine has an anti-nociceptive effect and dilates coronary arteries.
If Krebs cycle dysfunction is corrected, the patient is much calmer and anxiety has decreased, you can assume that more GABA is being formed. If there is increased anxiety, agitation, and poor sleep, glutamate may not be converting to GABA. If this is the case, B6 and P-5-P should be considered as indicated below.
In summary, you will locate an inhibited or weak muscle. Next, have the patient rebreathe their own air with a brown paper lunch bag. If the inhibited muscle strengthens, it implies that there is Krebs cycle dysfunction. In addition, you will want to check other muscles to get the big picture. This is indicated in the flow chart below. If rebreathing facilitates the inhibited muscle and does not inhibit a normal muscle, it is most likely just Krebs cycle dysfunction. If rebreathing facilitates the inhibited muscle and inhibits the supraspinatus, it is most likely Krebs cycle dysfunction and glutamate conversion to GABA. If rebreathing facilitates an inhibited muscle and inhibits a normal muscle, this implies that there is Krebs cycle dysfunction and inhibits a normal muscle ATP, which is not being converted to adenosine.
Rebreathing facilitates a conditionally inhibited muscle and:
l.Does not inhibit a normally facilitated indicator or supraspinatus
a. Krebs cycle and electron transport chain
i. Typically treat the small intestine Chapman’s reflex
2. Inhibits supraspinatus
a. Krebs cycle and glutamate conversion to GABA
ii. Typically treat the brain Chapman’s reflex 3.Inhibits normally facilitated indicator
a. Krebs cycle and ATP conversion to adenosine
iii. Typically treat the heart Chapman’s reflex Taking into consideration the evidence provided, it is
easy to conclude that mitochondria health and Krebs cycle function should be at the top of the list in systemic nutritional and physiological factors considered when treating a patient. Even if no other nutrition is considered, mitochondria and Krebs cycle should be to assure optimal treatment outcome and patient health.
Dr. Belli the current president of the International College of Applied Kinesiology graduated magna cum laude from Life Chiropractic College West in 1984. Dr. Belli is a Fellow of the American Board of Neurochemistry and Nutrition and a Diplomat of the American Chiropractic Association Council on Neurology. Additionally, Dr. Belli has spent the last 30 years researching and developing advanced systems of neurologically based Applied Kinesiology. You may contact Dr. Belli at [email protected].