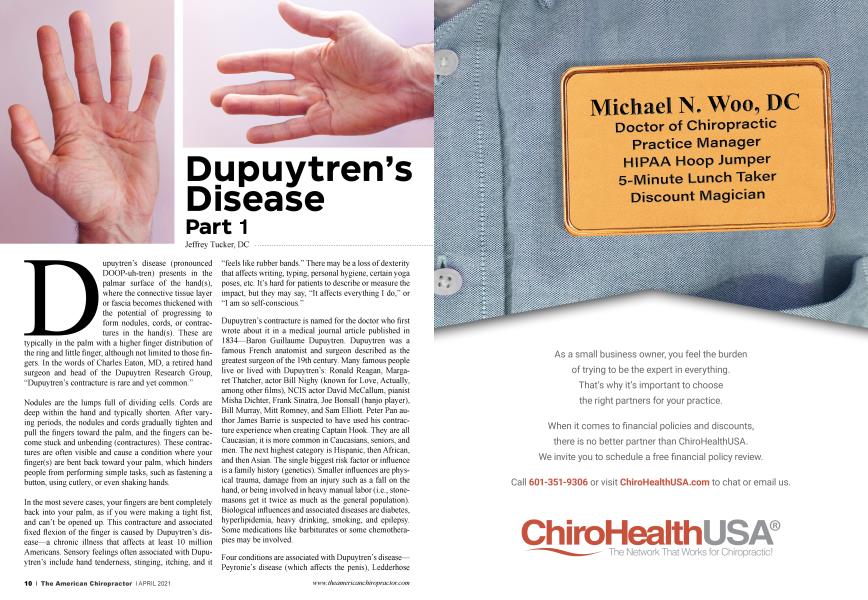
Dupuytren’s disease (pronounced DOOP-uh-tren) presents in the palmar surface of the hand(s), where the connective tissue layer or fascia becomes thickened with the potential of progressing to form nodules, cords, or contractures in the hand(s). These are typically in the palm with a higher finger distribution of the ring and little finger, although not limited to those fingers. In the words of Charles Eaton, MD, a retired hand surgeon and head of the Dupuytren Research Group, “Dupuytren’s contracture is rare and yet common.”
Nodules are the lumps full of dividing cells. Cords are deep within the hand and typically shorten. After varying periods, the nodules and cords gradually tighten and pull the fingers toward the palm, and the fingers can become stuck and unbending (contractures). These contractures are often visible and cause a condition where your finger(s) are bent back toward your palm, which hinders people from performing simple tasks, such as fastening a button, using cutlery, or even shaking hands.
In the most severe cases, your fingers are bent completely back into your palm, as if you were making a tight fist, and can’t be opened up. This contracture and associated fixed flexion of the finger is caused by Dupuytren’s disease—a chronic illness that affects at least 10 million Americans. Sensory feelings often associated with Dupuytren’s include hand tenderness, stinging, itching, and it “feels like rubber bands.” There may be a loss of dexterity that affects writing, typing, personal hygiene, certain yoga poses, etc. It’s hard for patients to describe or measure the impact, but they may say, “It affects everything I do,” or “I am so self-conscious.”
Dupuytren’s contracture is named for the doctor who first wrote about it in a medical journal article published in 1834—Baron Guillaume Dupuytren. Dupuytren was a famous French anatomist and surgeon described as the greatest surgeon of the 19th century. Many famous people live or lived with Dupuytren’s: Ronald Reagan, Margaret Thatcher, actor Bill Nighy (known for Love, Actually, among other films), NCIS actor David McCallum, pianist Misha Dichter, Frank Sinatra, Joe Bonsall (banjo player), Bill Murray, Mitt Romney, and Sam Elliott. Peter Pan author James Barrie is suspected to have used his contracture experience when creating Captain Hook. They are all Caucasian; it is more common in Caucasians, seniors, and men. The next highest category is Hispanic, then African, and then Asian. The single biggest risk factor or influence is a family history (genetics). Smaller influences are physical trauma, damage from an injury such as a fall on the hand, or being involved in heavy manual labor (i.e., stonemasons get it twice as much as the general population). Biological influences and associated diseases are diabetes, hyperlipidemia, heavy drinking, smoking, and epilepsy. Some medications like barbiturates or some chemotherapies may be involved.
"The diagnosis is primarily made by the history, visual analysis, and palpation."
Four conditions are associated with Dupuytren’s disease— Peyronie’s disease (which affects the penis), Ledderhose disease (which affects the bottom of the feet), frozen shoulder, and knuckle pads. The relationship between them is still not entirely clear, but having Dupuytren’s raises your chance of getting these conditions. Similarly, having any of these conditions makes it more likely you will get Dupuytren’s disease.
A diagnosis is primarily made by the history, visual analysis, and palpation. Plain film imaging or MRI of the hand and wrist is rarely necessary. With appropriate orthopedic testing, you should be able to rule out other soft-tissue pathology at the palm or wrist. Some doctors use diagnostic ultrasound to demonstrate the accuracy and landscape of the cross-sectional area of nodules, cords, and contractures. Ultrasonography can be used to measure enlargement or density within the palmar surface. Although electromyography (EMG) and nerve conduction studies (NCS) are considered the diagnostic gold standard for identifying and objectively classifying carpal tunnel syndrome (CTS), it’s not generally necessary for Dupuytren’s cases. Electromyography is useful to evaluate specific muscle weakness, and nerve conduction studies can pinpoint more specific sites of nerve involvement if the symptoms are complicated. Documentation includes noting the level of contracture determined for each finger and each finger joint measured by a goniometer.
Differential diagnosis
I have seen Dupuytren’s cases that have presented with cervical radiculopathy, pronator syndrome, thoracic outlet syndrome, compartment syndrome, and lateral and medial epicondylitis. Clinicians should consider local space-occupying lesions, including flexor tenosynovitis or ganglion cysts. Symptoms of peripheral neuropathy (nerve disease or damage to the peripheral nervous system) can confuse Dupuytren’s disease cases (for doctors and patients). If the patient has sensations described as burning, shooting, electric shock-like, throbbing, aching, or hands and feet falling asleep sensation, consider treating these symptoms appropriately.
What happens over time with Dupuytren disease?
It typically develops in both hands, with the ring finger and pinky finger most affected. In the first 10 years, one in 10 goes away, seven in 10 have little change, and two in 10 develop a bent finger. Most people have a mild version, but for the moderate-to-severe contractures, it can make daily activities difficult. Daily tasks that typically involve the entire hand (or both hands)—opening jars, driving, washing your face, carrying objects, shaking hands, certain kinds of household maintenance—become challenging or even impossible. Health problems may be associated with this disease, such as increased risk for cardiovascular disease, depression, thyroid disease, and diabetes. There is a reduced life expectancy and increased cancer risk, but the reasons are unknown.
Dupuytren’s is a fibrotic disease and shares cellular and molecular pathways with pulmonary fibrosis, renal interstitial fibrosis, liver fibrosis, and arteriosclerosis. The fascia beneath the skin is the most affected. Dupuytren’s disease causes the fascia to become inflamed and diseased, resulting in a tightening cord that pulls the finger(s) closed.
I don’t usually see a Dupuytren’s case in the inflammatory phase as we think of it. Rather, I see the patient with fascia pain and deformation, probably resulting from a noninflammatory, degenerative process. Initial insults (acute injury from a fall, repetitive chronic overload from manual labor) that occurred in the past may have caused an acute local inflammatory reaction, along with some yet unknown molecular or cellular disease that results in a breakdown of the inflammatory process and a disorganized healing process that fails to regenerate “normal” tissue.
In part two of this article, I will discuss treatment therapies for Dupuytren’s disease.
Dr. Jeffrey Tucker is the current president of the ACA Rehab Council. Dr. Tucker practices in Los Angeles, CA. His website is www. DrJeffreyTucker.com