Swayback Posture and Therapy
POSTURE
Jeffrey Tucker
DC
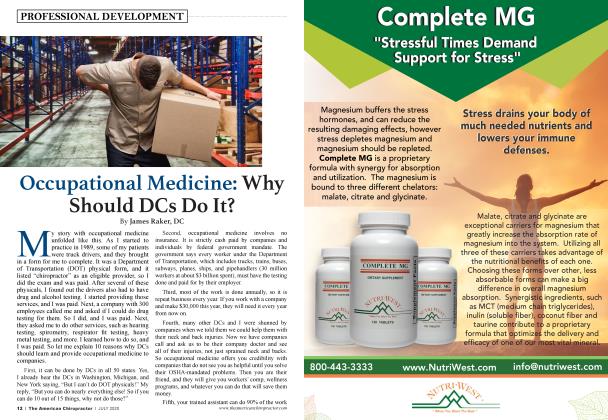
The term “swayback” refers to a flattened low lumbar area. The concave curve of the lower spine is much higher and in the lower thoracic spine; the pelvis is tilted posteriorly; the plumb line of the greater trochanter is anterior to the lateral malleolus, revealing the hips and pelvis swayed forward in the sagittal plane (Kendall 2005); and the rib cage is swayed backward in the sagittal plane (Sahrmann 2002).
Swayback posture is common in individuals who are sedentary and sit for prolonged periods, older adults with weak gluteal muscles, runners, and ballerinas (Sahrmann 2002). Those with swayback frequently present to chiropractors with chronic low back pain.
“Lordotic posture” refers to the excessive concave lumbar spine. The pelvis is tilted anteriorly, and, in both lordotic and ideal postures, the greater trochanter is over the lateral malleolus. Hip flexor tightness (iliopsoas, quadriceps, vastus) is common with lordotic posture (Kendall 2005). Visually, the pelvic bowl dips anteriorly, raising the body’s center of gravity.
Lordotic postures (Lee, CM, et al. 2001) and swayback can lead to reduced proprioceptive stability. Wearing high heels should be avoided with excessive lumbar lordosis.
How to Identify Swayback Posture from the Ground Up:
• Neutral ankle joint
• Hyperextended knees and hips (femurs create a joint with hyperextended knees and hips)
• Posterior pelvic tilt
• Anterior deviation of the pelvis over the lateral malleoli
• Flattened lower lumbar spine
• Gluteals may look flattened
• Caved chest
• Long kyphosis (backward curve of the thoracic spine, also known as “hunchback” or rounded upper back) in the posteriorly displaced upper trunk
• Forward head posture
Muscle length evaluation reveals short hamstrings (patient’s perception is “tight” hamstring) and internal oblique muscles with lengthened psoas and external oblique muscles (Kendall 2005).
Muscle strength evaluation reveals dominance of the rectus abdominis over the external obliques (Sahrmann 2002). The gluteals may be atrophied and test as weak.
Palpation of the lower rectus abdominis close to the pubic bone attachments often reveals tenderness, tightness, or trigger points. This shortening contributes to the posterior pelvic tilt and the caving of the chest. We should be able to diagnose swayback versus increased lumbar lordosis by the forward pelvis and the upper torso backward shift (Kendall 2005).
Gait analysis reveals hamstring dominance over the gluteals to extend the hip. The posterior pelvis tilt puts the gluteals in an abnormal length, causing them to be inhibited and allowing the hamstrings to take over as the prime movers for hip extension. This alters the length (origin and insertion) of the hamstrings, and the extension they create at the hip puts a torque on the femur, causing the head of the femur to move forward in the hip socket (Sahrmann 2002). Time and repetition of walking or running loads can produce significant wear and tear on the anterior area (ligaments, bursa, etc.) of the hip joint and may cause groin pain or hip symptoms. There also will be excess strain on the hamstring tendons especially at the ischial attachments.
Common overuse injuries related to faulty swayback posture include labral tears at the hip, lowback pain, plantar fasciitis, iliopsoas bursitis and tendinopathy, recurrent hamstring strain, and shoulder impingement (Sahrmann 2002).
Management:
Manual therapy: Clinically, our hands will never go out of style, and we need to restore physiological vertebral movement and perform manipulation of the apophyseal joints. These patients are stiff especially in the thoracic spine.
Deep Muscle Stimulator: I have observed that the newly developed deep muscle massager DMS-Dr Fuji DMS pro6 developed by Dr. Fuji is an excellent complement and “patient pleaser” compared to all other handheld vibration-percussion devices Fve tried, especially for fascial dysfunction. Dr. Fuji was able to manufacture a cordless, rechargeable, and ergonomically designed handheld instrument. The DMS-Dr. Fuji DMS pro6 device comes with three separate heads for the applicator and offers five energy intensity settings.
There are two probable primary effects of the deep muscle massager:
1. Direct reaction to the mechanical stimulation.
2. Indirect stimulation triggering cellular and biochemical processes based on triggering a reactive system.
Direct effects may include the following:
Normalization of the muscle tone through stimulation of the muscle spindle and the Golgi apparatus of the muscle tendon.
Pain overlay based on the gate-control principle (Melzack and Wall) with parallel endorphin release by the stimulation of the skin’s pressure and touch receptors.
Stimulation of cellular activity and changes in cell-membrane permeability caused by direct mechanical stress in the cell wall.
Increased cellular metabolism due to changes in the membrane permeability, e.g., by opening the glutamate channels.
Release of substance P, a neurotransmitter and pain mediator, into the tissue with subsequent nerve habituation and, with that, reduction of the pain threshold.
Increased cellular activity.
Mechanotransduction, i.e., the process of converting physical forces into biochemical signals subsequently integrated into a cellular response (Iqbal & Zaida 2005; Vogel 2006).
I specifically use the DMS-Dr. Fuji DMS pro6 for postural distortions to increase venous and arterial flow to the tight muscles and reawakening of underactive muscles. The deep muscle stimulator (DMS) vibration also is likely to increase metabolite transport into the disc to complement increased imbibition, increase glycosaminoglycans, and increase potassium, calcium, magnesium, iron, and sodium nutrient flow in channels between the vertebral end plates and the disc. The new DMS device does more than assist in breaking up adhesions and scar tissue; it likely offers mechanoreceptor activation around facet joints (type II) and helps pain mediation by blocking the pain-spasm-pain cycle.
Postural Retraining: This is patient “awareness” of the dysfunction while helping the patient find a more neutral or “less threatening,” “more stable,” “more breath,” “more movement,” or whatever you want to call it “position.” Be sure they lengthen the torso through the top of the head and elongate the spine. For patients in pain, this will calm the muscles and remove the effects of the spine’s poor position (McGill 2007). My goal is to reduce the kyphosis.
Specific Exercises: I use ELDOA exercises to increase IVD space height and facilitate imbibition. The ELDOA exercises complement the DMS and the postural changes I am trying to make to increase the length and size of the discs and spinal canals. Other specific exercises include side planks and hand/forearm-to-toes planks. These will shorten and strengthen the external obliques while maintaining length in the internal obliques and rectus abdominis. Bridging and standing single-leg march in place performed slow with arm drivers strengthen the gluteals and psoas while increasing hip mobility and elongating the spine.
Exercise goals:
• Increase mobility at the hips, specifically hip flexion.
• Increase strength of the gluteus maximus.
• Decrease length of the external obliques and decrease dominance of the rectus abdominis.
• Strengthen the short hip flexors (psoas).
• Create mobility in the thoracic spine.
I have patients avoid traditional curl-ups because they continue to build dominance of the rectus abdominis.
Treatment Summary
When working with swayback patients, it is important to emphasize postural cues, as well as employ DMS for fascial therapy and corrective exercises. I constantly remind the patient to stand in better alignment—active arch (short foot), relaxed knees, pelvis neutral, chest open and in an elongated “tall” position, palms at sides with thumbs facing forward, and no forward head posture.
Jeffrey Tucker, DC, DACRB, practices in West Los Angeles, CA. Dr. Jeffrey Tucker is the current president of the ACA Rehab Council. The Rehab Council will have its annual conference March 13-14, 2021 in Orlando, FL. The website to register is www.ACARehabCouncil.org. Dr. Tucker's website is www.DrJeffreyTucker.com