Weight-Bearing vs. Non-Weight Bearing Orthotic Casting: A Practical Approach
ORTHOTICS
PERSPECTIVE
Kevin Wong
DC
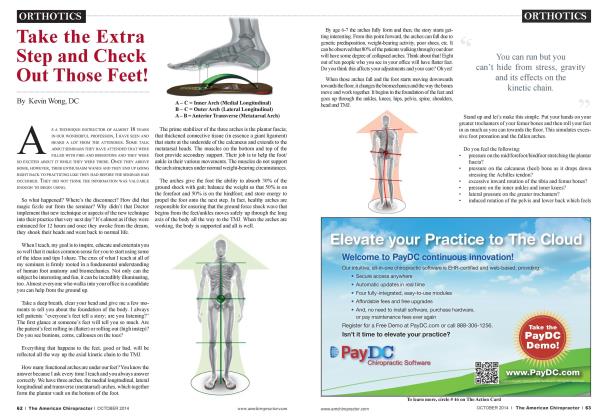
The feet/ankles are often overlooked by health care professionals when patients present with musculoskeletal pain. I like to point out that the farther away from the feet the patient’s pain is, the more the practitioner forgets to check the feet. It is astonishing how much pain in the spine, pelvis, hips, and knees are due to unhealthy feet. The three functional arches that make up the plantar vault stop developing after age 6-7. After that, foot problems can begin. 80-87% of the time, the result is arch collapse/flattening and excessive or over-pro nation. In 3-5% of patients, their feet supinate or roll outward. In either case, foot stability is compromised.
Custom made orthotics are one of the most popular options to treat flat feet. Numerous health care providers use orthotics to help their patients’ feet feel less pain. The idea behind the orthotic is simple: support the arches where the arches are lacking. But here is the issue: What is the best way to capture the support the feet need and how do we make them? Some practitioners believe that non-weight bearing is the best way as it has been medical convention for years.
Others believe that weight-bearing casting is more accurate. Whom do you believe? This is a valid and frequently asked question I get a lot in my lectures and from patients. After all, when a patient questions you and says the “Real Foot Doctor makes them non-weight bearing”, you need to be able to support your answer. It’s our job to un-muddy the waters. Let’s talk about this and see what you think once we are done.
For many years, non-weight-bearing casting has been the conventional medical way of making orthotics. This method normally has the patient sitting or lying down with their feet in a relaxed position. The practitioner will then push on the metatarsal region of the foot in an attempt to place the foot at a 90-degree angle with the tibia. This is subtalar neutral (or a neutral position of the talus bone). Plaster Paris strips are then applied around the foot to make a “negative impression”. A plaster paris cast is formed, which essentially renders a 3-D model of the feet.
In some cases, the non-weight bearing casting takes the form of the practitioner having the patient sitting on a chair with their knees at 90 degrees and their feet on the ground. Foam is placed under their feet and the practitioner pushes down on their knee and this passive force pushes the foot into the foam and creates an impression.
Recentfy, a popular and more cutting edge method of non-weight bearing casting has the patient sitting or lying down again. But this time, the practitioner holds each foot in subtalar neutral and places a portable foot scanner against it. The scanner makes a 3-D image of each foot. The images are then used to make the custom orthotic.
The idea behind these non-weight bearing casting methods is that if the patient has arch support when they are non-weight bearing, then the cast made will in effect “mirror’ that arch support. The orthotic produced from this cast/scan will then provide the foot with that same support underneath it when the patient stands on it.
The human body is a biomechanical wonder. Each body part is intimately related to each other. Unfortunately, most patients and health care providers aren't trained to look at the body this way. Health care is often doled out into pieces with pain being the motivator in seeking out a particular practitioner to go after that area of the body. The feet work within a certain homeostasis where all 3 arches must have support to provide a stable base for the feet and the rest of the body. Since the 3 arches form a triangle of support for the bottom of the feet, once we lose one of the sides, it won't be long before the other two are compromised. Understanding that we have 3 functional arches and NOT just one is a fundamental concept of foot support that escapes most patients and people we come in to contact with.
When a non-weight bearing cast is made with any of the techniques described above, the fundamental issue is that the subtalar foot position is NEVER present during the gait cycle. Think about that for a second! The mainstream medical and conventional way feet have been casted for many years holds the foot in a position that the patient will never be in when they are standing on top of the orthotic that has been made for them.
The other glaring problem here is that non-weight bearing casting does not account for all 3 of the arches. This casting method is mostly for addressing the medial longitudinal arch, which is the only arch most humans in the world think exists under their feet. The 3 arches are not being accounted for so the support is incomplete. At times, I have seen small pads placed on top of the metatarsal area of the orthotic to account for the transverse arch, but this is not standard. Metatarsal pads tend to be used only when a patient requests more support or continues to complain of pain in the ball of their foot.
When we are walking, the ground transmits about 5G's of shock to the calcaneus bone. The types of orthotics made from these casts tend to be rigid or semi-rigid in nature. This hard object under people's feet will actually transmit 5-7 times more shock to the feet and the rest of the joints than normal. They are often so uncomfortable, patients can not wear them. It can be very frustrating and painful for patients to force themselves to wear rigid orthotics.
The flip side of the coin has to do with those who utilize weight-bearing casting or scanning. Here, the practitioner has the patient stand or step on to foam molds or a digital foot scanner. The concept here is that the patient is now full weight-bearing, a position that is seen with every "foot flat” portion of the gait cycle. Even though the patient's full body weight is on their feet and we see the feet at their flattest, the impression is then analyzed, specific measurements are made and orthotics are produced for each foot. Each foot has its' own arch issues, which will be addressed by the orthotic that is made from the weight-bearing image.
Quite simply, this method is easier because the patient just needs to stand on something with their eyes looking forward and their arms at their sides. This method also produces orthotics that have all 3 of the arches so there is full support for both feet. The orthotics produced are also flexible so that when the patient stands on them, they are extremely comfortable and have a break-in period of about 2-3 weeks.
As a Chiropractic clinician treating patients daily, I have found the weight-bearing, 3 arch, flexible orthotics consistently yield positive results for patients in terms of foot/arch support, pain reduction and improvement in biomechanical stability.
Kevin Wong, DC, is a 1996 summa cum laude graduate of Palmer College of Chiropractic West. A past instructor of chiropractic technique for the college, he is currently part of the adjunct faculty. Dr. Wong is also a past lecturer and instructor for the International Chiropractic Association of California. Currently, he is in full-time practice in Orinda, California, and has been a speaker for Foot Levelers for many years.