Body Sway, Proprioception, and Spinal Curves
SCOLIOSIS
BODY SWAY
Part 2: Pathology or Physiology?
(Continuation of the article published in the Volume 40, Number 8, 2018)
Richard M. Opper
DC
"In effect, the muscle activity that bent the spine in the frontal plane also flattened it in the sagittal plane."
"The pelvis is a mechanism for balance” [Gray], and the spinal column complex is an organ of balance. Adolescent Idiopathic Scoliosis (AIS) appears to be an exquisite demonstration of a primitive and powerful neuromuscular reflex using the spinal column complex to avert a challenge to survival— imbalance. Thousands of researchers and clinicians over 200 years or more are all correct; no known pathology causes AIS and, more than likely, there is no unknown pathology as well.
The spinal column and its attendant structures, including muscle, fascia, ligament, capsular tissue, intervertebral disc, neural organs, and bone, respond to intentional and autonomic motor commands. Cognitive motor commands facilitate various motions and postures as needed to ambulate and perform tasks. Mechanoreceptor commands originating within the spinal column complex facilitate upright balance [1]. In other words, we have conscious control over the shape of our spine when performing tasks, but the spinal column complex has autonomic control over its shape to ensure verticality. Our skeleton is inherently unstable because the architecture of each bony component is arcuate, necessitating continual proprioceptive monitoring. The ability of the neuromuscular spinal reflex system to alter the sagittal and frontal plane curves, as well as the pelvic tilt to compensate for stresses, supports upright balance. The arched shape of the three primary sagittal curves allows for modification by the central nervous system to regulate standing balance as directed by the resident proprioceptors in the spinal column complex. The most powerful response of the primitive nervous system occurs when it attempts to correct imbalance by contracting and relaxing the deep muscles of the back.
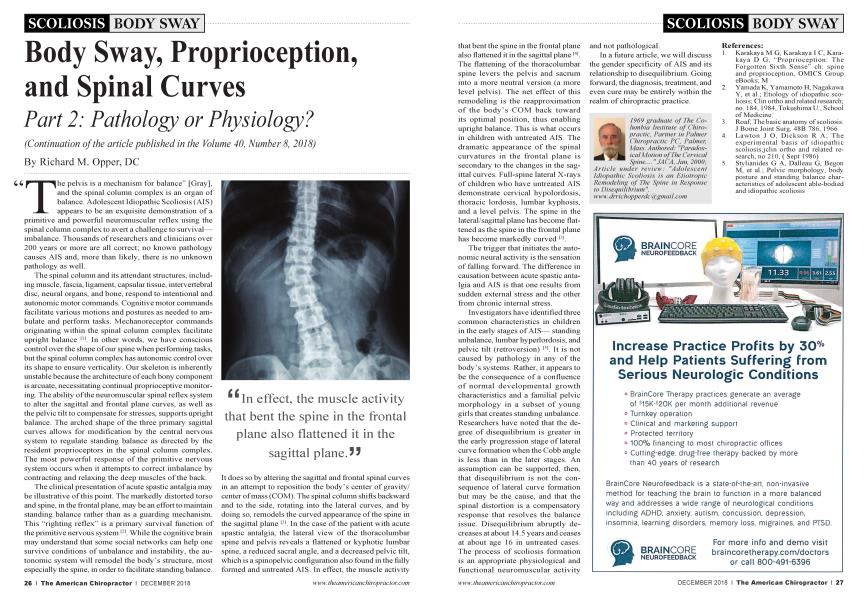
The clinical presentation of acute spastic antalgia may be illustrative of this point. The markedly distorted torso and spine, in the frontal plane, may be an effort to maintain standing balance rather than as a guarding mechanism. This “righting reflex” is a primary survival function of the primitive nervous system[2]. While the cognitive brain may understand that some social networks can help one survive conditions of unbalance and instability, the autonomic system will remodel the body’s structure, most especially the spine, in order to facilitate standing balance. It does so by altering the sagittal and frontal spinal curves in an attempt to reposition the body’s center of gravity/ center of mass (COM). The spinal column shifts backward and to the side, rotating into the lateral curves, and by doing so, remodels the curved appearance of the spine in the sagittal plane [3]. In the case of the patient with acute spastic antalgia, the lateral view of the thoracolumbar spine and pelvis reveals a flattened or kyphotic lumbar spine, a reduced sacral angle, and a decreased pelvic tilt, which is a spinopelvic configuration also found in the fully formed and untreated AIS. In effect, the muscle activity that bent the spine in the frontal plane also flattened it in the sagittal plane[4]. The flattening of the thoracolumbar spine levers the pelvis and sacrum into a more neutral version (a more level pelvis). The net effect of this remodeling is the reapproximation of the body’s COM back toward its optimal position, thus enabling upright balance. This is what occurs in children with untreated AIS. The dramatic appearance of the spinal curvatures in the frontal plane is secondary to the changes in the sagittal curves. Full-spine lateral X-rays of children who have untreated AIS demonstrate cervical hypolordosis, thoracic lordosis, lumbar kyphosis, and a level pelvis. The spine in the lateral/sagittal plane has become flattened as the spine in the frontal plane has become markedly curved [3].
The trigger that initiates the autonomic neural activity is the sensation of falling forward. The difference in causation between acute spastic antalgia and AIS is that one results from sudden external stress and the other from chronic internal stress.
Investigators have identified three common characteristics in children in the early stages of AIS— standing unbalance, lumbar hyperlordosis, and pelvic tilt (retroversion) [5]. It is not caused by pathology in any of the body’s systems. Rather, it appears to be the consequence of a confluence of normal developmental growth characteristics and a familial pelvic morphology in a subset of young girls that creates standing unbalance. Researchers have noted that the degree of disequilibrium is greater in the early progression stage of lateral curve formation when the Cobb angle is less than in the later stages. An assumption can be supported, then, that disequilibrium is not the consequence of lateral curve formation but may be the cause, and that the spinal distortion is a compensatory response that resolves the balance issue. Disequilibrium abruptly decreases at about 14.5 years and ceases at about age 16 in untreated cases. The process of scoliosis formation is an appropriate physiological and functional neuromuscular activity and not pathological.
In a future article, we will discuss the gender specificity of AIS and its relationship to disequilibrium. Going forward, the diagnosis, treatment, and even cure may be entirely within the realm of chiropractic practice.
References:
1. Karakaya M G, Karakaya I C, Karakaya D G; “Proprioception: The Forgotten Sixth Sense” ch: spine and proprioception, OMICS Group eBooks; M
2. Y amada K, Y amamoto H, Nagakawa Y, et al.; Etiology of idiopathic scoliosis; Clin ortho and related research; no. 184, 1984, Tokushima U., School of Medicine.
3. Roaf; The basic anatomy of scoliosis. J Borne Joint Surg. 48B:786, 1966
4 Lawton J O, Dickson R A; The experimental basis of idiopathic scoliosis;jclin ortho and related research, no 210, ( Sept 1986)
5. Stylianides G A, Dalleau G, Begon M, et al.; Pelvic morphology, body posture and standing balance characteristics of adolescent able-bodied and idiopathic scoliosis
1969 graduate of The Copractic, Chiropractic Institute Partner in PC, of Palmer Palmer, ChiroMass. Authored: "Paradoxical Motion of The Cervical Spine.... " J AC A, Jan, 2000; Article under review: "Adolescent Idiopathic Scoliosis is an Etiotropic Remodeling of The Spine in Response to Disequilibrium ". www. drrichopperdcagmail. com