THE FOUR (often confusing) TYPES OF PMS
INTEGRATIVE HEALTH
Howard Loomis
A disease is a pathological process that can be identified with objective evidence. It may be seen on an MRI or X-ray, heard through a stethoscope, identified on an EKG, or perhaps be suspected by palpating a breast lump or enlarged prostate gland. A disorder is a normal physiological process that is going too fast, too slow, or otherwise out of time with another normal body process.
Despite scientific advances in medicine, one of the most perplexing disorders in modern society continues to be premenstrual syndrome (PMS). The problem lies in the seemingly endless list of associated symptoms that defy classification as a disease entity and come and go with each luteal phase of the menstrual cycle.
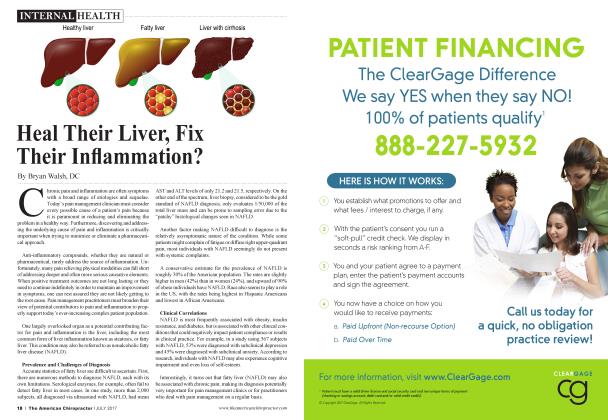
Emotional and Behavioral Symptoms Appetite changes Trouble falling Mood swings and and food cravings asleep (insomnia) Crying spells irritability or anger Social Tension or anxiety Depressed mood withdrawal Poor concentration Physical Signs and Symptoms Constipation Joint or Weight gain related or diarrhea muscle pain Fatigue to fluid retention Abdominal Breast bloating tenderness Acne flare-ups Headaches Downloaded from Mayo Clinic website March 21, 2017
Due to lack of clinical success, modern emphasis has shifted away from understanding the normal physiological pathways of menstruation to treatment of coexisting conditions, particularly anxiety and depression. Studies indicate that women with premenstrual syndrome usually present with both physical and mood symptoms, with irritability as the hallmark symptom. In addition, PMS is associated with a high rate of major depressive disorders (MDD).1
Consistent with previous studies, another study suggests an increased prevalence of MDD and other disorders among women with newly diagnosed endocrine disorders, providing further evidence suggesting that women with endocrine abnormalities may be at increased risk of depression and/or anxiety disorders.2
What does chiropractic offer in helping women cope with what is often mistakenly assumed to be “normal” for most women? The previous references and all of those found in my book The Enzyme Advantage for Women provide clues well worth considering. There are now four totally separate approaches
based on physiological and nutritional causes available to help you assist your female patients.
PMS-A: THE HIGH-ANXIETY, IRRITABLE TYPE
Eighty percent of women with PMS are predominantly anxiety related and are driven by excess estrogen, a central nervous system stimulant. Alternatively, high estrogen levels may actually be related to a deficiency in progesterone, resulting in a high estrogen-to-progesterone ratio—not enough progesterone to quiet things down.
Symptoms of anxiety may also be the result of the body’s inability to break down estrogen, due to poor liver function or vitamin B deficiency.
Then there’s calcium. Fifty percent of calcium in the extracellular fluids is bound to protein, which means that in order for the body to absorb calcium, these women have to ingest, digest, and absorb protein. As protein levels go down, so do calcium levels.
One of the cardinal signs of a calcium deficiency is irritability progressing slowly to minor numbness or tingling of the fingers, muscle (menstrual) cramps, lethargy, and poor appetite. This reflects the low total calcium, which causes irritability and anxiety, accompanied by low ionized calcium, which is needed to prevent cramping.
Vitamin D supplementation may help improve calcium levels, but it does not address protein deficiency, and if you don’t have the protein to hold the calcium, it won’t do any good.
PMS-C: THE TYPE-A PERSONALITY SUGAR BEAR
Approximately 40% of women with PMS symptoms present with problems related to carbohydrate cravings. This is often due to increased responsiveness to insulin. The “sugar bear” consumes excessive amounts of shnple sugar. She also may consume so-called sugar substitutes (artificial sweeteners), which the body cannot digest and therefore provide zero calories.
Foremost on the list of this young woman’s problems is that refined sugars that are absorbed into file body necessitate the
use of important alkaline minerals, such as potassium and magnesium, and even sodium, along with B vitamins, to metabolize them. This reduces the availability of these key minerals and vitamins for more important functions.
The result is in stress to the body, particularly the respiratory system and the
kidneys, setting off the fight-or-flight cascade, and depleting stored energy sources for important body functions.
These young women are susceptible to adrenal exhaustion because of continued sympathetic stimulation, and because of alkaline mineral deficiency. Hence, they don’t have a lot of lasting energy. They just don’t have the adrenalin to keep them going.
Meanwhile, all of this stress causes constriction of the blood vessels that serve the body’s organs, particularly the kidneys. Thus, the kidneys’ ability to clean the blood is diminished, resulting in increased incidence of allergies, as well as back pain due to involuntary muscle contractions emanating horn the stressed kidneys.
Back pain and allergies are very often the symptoms that will drive sugar bears into the doctor’s office because their kidneys aren’t cleaning their blood adequately.
■ " Such a regimen can take the hit and miss out of PMS treatment. It’s all about giving the body what it needs, and treating each woman as an individual, with individual needs. There’s no magic bullet. J J
PMS-H: THE
SLOW METABOLISM TYPE
This group of symptoms affects about 60% of women with PMS. Signs and symptoms are predominantly bloating and edema, increased levels of ACTH (the stress hormone), and increased aldosterone secretion to preserve water and salt by the kidneys.
In other words, they’re holding water and it’s leaking out into the tissues, so they have edema.
These women are under chr onic stress and, as a result, they suffer from what appeals to be hypothyroidism—their thyroid gland is overworked and unable to produce enough thyroxin to keep them going. There’s your slow metabolism.
Their calcium levels may be adequate to prevent muscle cramping fr om progressing to numbness and tingling. However, there is inadequate stomach acid, and either poor protein ingestion or digestion, along with biliary stress, even if their gallbladder has been removed. This is because the bile is coming fr om the liver; the gallbladder just stores it.
Protein digestion creates acidity, and the biliary distress is due to the lack of stomach acid needed to thin bile out and get it flowing.
This young woman needs supplemental food enzymes to enhance protein and fat digestion, heavy-ended on lipase, as well as fatty acids and calcium and magnesium. All of this is aimed at nutritionally supporting her thyroid gland and improving her metabolic rate.
PMS-D: THE ANTACID OR PROTON PUMP INHIBITOR USER
On the matter of what has been termed PMS-D, only about 5% of PMS sufferers are primarily affected by depression related to excessive progesterone, a central nervous system depressant. Nutritional supplementation is of little help in this situation, and, clearly, treatment of clinical depression is beyond my expertise.
Nevertheless, my experience has been that having the symptoms associated with PMS following every ovulation in each menstrual cycle can be stressful if not debilitating.
In that regai d, there is a digestive syndrome intimately related to a large paid of the female population. Recall that stress irritates the lining of the stomach and is
responsible for the symptoms of what has been called excess stomach acid—i.e., heartburn, etc. However—and here’s the rub—it is impossible for the body to make excess stomach acid! The term itself is a misnomer. I wrote about GERD (think disorder, not disease) in my last article.
The symptoms of heartburn do not come h orn excess stomach acid. Rather, this burning sensation occurs when stomach acid irritates the protective mucosal lining of the stomach wall. Preventing or reducing the formation of stomach acid with a proton pump inhibitor can be a good thing—for a lhnited time, to give the mucosal lining time to heal.
The problem is that proton pump inhibitors have become the treatment of choice for all digestive issues and reports of side effects are mounting, including evidence of spontaneous fractures and kidney disease, to mention just two.
A final word about depression
PMS-D has been used as a marketing tool by the pharmaceutical industry for certain birth control pills allegedly aimed at helping people with PMS-related depression. European medical societies have rejected this ffom the beginning. Why? Because there is no separate group of PMS sufferers who are more susceptible to depression.
■ " Depression is the result of the degenerative process. It all comes down to stress.
Quite simply, when any woman suffers from PMS symptoms long enough, she is going to become depressed. Depression is the result of the degenerative process. It all comes down to stress.
Such a regimen as recommended in this article can take the hit and miss out of PMS treatment. It’s all about giving the body what it needs, and heating each woman as an individual with individual needs. There’s no magic bullet.
References:
1. The Epidemiology of Premenstr ual Syndrome, Primary Psychiatry December 1, 2004
2. World JBiol Psychiatry. 2010 Dec;ll(8):991-6.
Dr. Loomis has an extensive background in enzymes and enzyme supplements. He is the founder and president of the Food Enzyme Institute. His extensive knowledge of physiology, biochemistry, and enzymology has made him a sough t-after speaker and a prolific writer. The Food Enzyme Institute offers seminars to healthcare practitioners around the country. Dr. Loomis published ENZYMES: The Key to Health in 1999. He also co-authored andpublished The Enzyme Advantage: For Healthcare Providers and People Who Care About Their Health in 2015, and The Enzyme Ach’antage for Women in 2016, with respected medical journalist Arnold Mann. Contact info: 6421 Enterprise Lane, Madison, WI 53719 customer serviceTifoodenzymeinstitule.com, 800-662-2630.