Coccyx Pain and Treatment Part One
TECHNIQUE
A surprising number of people from distant places have contacted me for advice about, and for treatment of, coccyx-area pain—a pain that can be constant and severe. It commonly results from a traumatic onset, such as a fall or direct blow from a sports injury, or prolonged and repeated pressure to the area from sitting (an improper position or hard-surface chair). Mothers sometimes present with coccyx-area pain after childbirth, perhaps because during the last trimester of childbirth, the coccyx becomes more mobile, allowing for greater multidirectional movements. With my patients who have presented with a history of trauma, I have not seen many overt coccyx fractures on X-ray, but I suspect bone bruising and microfractures (not seen on X-rays). X-ray can help detennine dislocation at the sacrococcygeal joint (usually an anterior coccyx) causing significant pain and discomfort during sitting, sitting to standing, and even walking. Any trauma or repetitive irritation can cause damage to the attached musculoligamentous tissues with an inflammatory response, periostitis, and eventual osteoarthritis of the sacrococcygeal joint.
Pelvic floor stability (preventing inferior sagging of the intrapelvic contents), maintaining urinary and fecal continence, and diaphragmatic breathing continue to be hot topics for those interested in rehab and sports performance. The pelvic floor is often an overlooked area for chronic pain patients. Because the muscles originating from the posterior coccyx include the gluteus maximus and strands of biceps femoris, which is often continuous with the sacrotuberous ligaments, it is important to at least examine this area.
The coccyx is not just a postage stamp-size area that can become extremely painful. If we follow Tom Meyers (Anatomy Trains) as he describes how “everything is connected to everything,” the Superficial Back Line includes the plantar tissues, the triceps surae, the hamstrings and sacrotuberous ligament, the erector spinae, and the epicranial fascia. The Superficial Back Line functions in movement to extend the spine and hips, and flex the knee and ankle. Posturally, the Superficial Back Line maintains the body in standing.
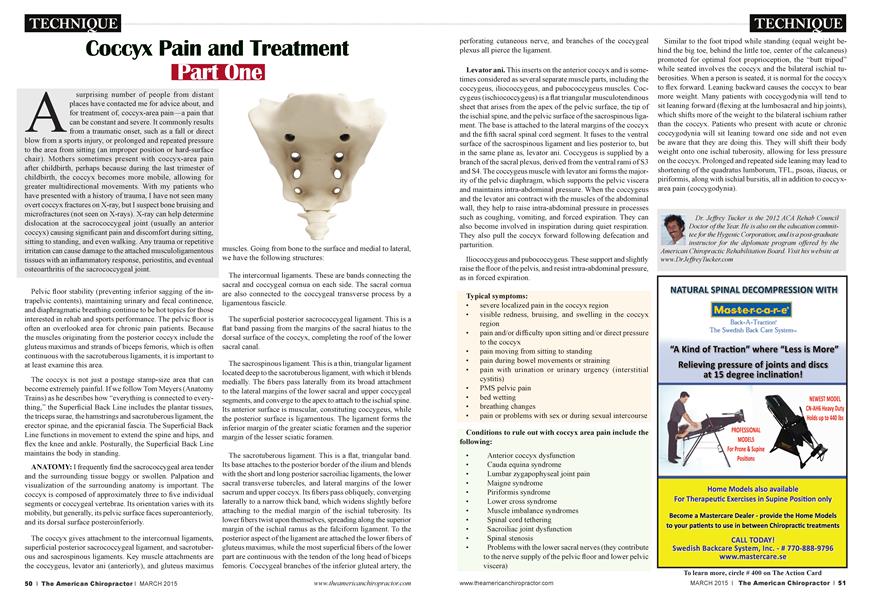
ANATOMY: I frequently find the sacrococcygeal area tender and the surrounding tissue boggy or swollen. Palpation and visualization of the surrounding anatomy is important. The coccyx is composed of approximately three to five individual segments or coccygeal vertebrae. Its orientation varies with its mobility, but generally, its pelvic surface faces superoanteriorly, and its dorsal surface posteroinferiorly.
The coccyx gives attachment to the intercomual ligaments, superficial posterior sacrococcygeal ligament, and sacrotuberous and sacrospinous ligaments. Key muscle attachments aie the coccygeus, levator ani (anteriorly), and gluteus maximus
muscles. Going from bone to the surface and medial to lateral, we have the following structures:
The intercomual ligaments. These are bands connecting the sacral and coccygeal cornua on each side. The sacral cornua aie also connected to the coccygeal transverse process by a ligamentous fascicle.
The superficial posterior sacrococcygeal ligament. This is a flat band passing from the margins of the sacral hiatus to the dorsal surface of the coccyx, completing the roof of the lower sacral canal.
The sacrospinous ligament. This is a thin, triangular ligament located deep to the sacrotuberous ligament, with which it blends medially. The fibers pass laterally from its broad attachment to the lateral margins of the lower sacral and upper coccygeal segments, and converge to the apex to attach to the ischial spine. Its anterior surface is muscular, constituting coccygeus, while the posterior surface is ligamentous. The ligament forms the inferior margin of the greater sciatic foramen and the superior margin of the lesser sciatic foramen.
The sacrotuberous ligament. This is a flat, triangular band. Its base attaches to the posterior border of the ilium and blends with the short and long posterior sacroiliac ligaments, the lower sacral transverse tubercles, and lateral margins of the lower sacrum and upper coccyx. Its fibers pass obliquely, converging laterally to a narrow thick band, which widens slightly before attaching to the medial margin of the ischial tuberosity. Its lower fibers twist upon themselves, spreading along the superior margin of the ischial ramus as the falciform ligament. To the posterior aspect of the ligament are attached the lower fibers of gluteus maximus, while the most superficial fibers of the lower part are continuous with the tendon of the long head of biceps femoris. Coccygeal branches of the inferior gluteal artery, the perforating cutaneous nerve, and branches of the coccygeal plexus all pierce the ligament.
Levator ani. This inserts on the anterior coccyx and is sometimes considered as several separate muscle parts, including the coccygeus, iliococcygeus, and pubococcygeus muscles. Coccygeus (ischiococcygeus) is a flat triangular musculotendinous sheet that arises from the apex of the pelvic surface, the tip of the ischial spine, and the pelvic surface of the sacrospinous ligament. The base is attached to the lateral margins of the coccyx and the fifth sacral spinal cord segment. It fuses to the ventral surface of the sacrospinous ligament and lies posterior to, but in the same plane as, levator ani. Coccygeus is supplied by a branch of the sacral plexus, derived from the ventral rami of S3 and S4. The coccygeus muscle with levator ani forms the majority of the pelvic diaphragm, which supports the pelvic viscera and maintains intra-abdominal pressure. When the coccygeus and the levator ani contract with the muscles of the abdominal wall, they help to raise intra-abdominal pressure in processes such as coughing, vomiting, and forced expiration. They can also become involved in inspiration during quiet respiration. They also pull the coccyx forward following defecation and parturition.
Iliococcygeus and pubococcygeus. These support and slightly raise the floor of the pelvis, and resist intra-abdominal pressure, as in forced expiration.
Typical symptoms:
• severe localized pain in the coccyx region
• visible redness, bruising, and swelling in the coccyx region
• pain and/or difficulty upon sitting and/or direct pressure to the coccyx
• pain moving from sitting to standing
• pain during bowel movements or straining
• pain with urination or urinary urgency (interstitial cystitis)
• PMS pelvic pain
• bed wetting
• breathing changes
• pain or problems with sex or during sexual intercourse
Conditions to rule out with coccyx area pain include the following:
• Anterior coccyx dysfunction
• Cauda equina syndrome
• Lumbar zygapophyseal joint pain
• Maigne syndrome
• Piriformis syndrome
• Lower cross syndrome
• Muscle imbalance syndromes
• Spinal cord tethering
• Sacroiliac joint dysfunction
• Spinal stenosis
• Problems with the lower sacral nerves (they contribute to the nerve supply of the pelvic floor and lower pelvic viscera)
Similar to the foot tripod while standing (equal weight behind the big toe, behind the little toe, center of the calcaneus) promoted for optimal foot proprioception, the “butt tripod” while seated involves the coccyx and the bilateral ischial tuberosities. When a person is seated, it is normal for the coccyx to flex forward. Leaning backward causes the coccyx to bear more weight. Many patients with coccygodynia will tend to sit leaning forward (flexing at the lumbosacral and hip joints), which shifts more of the weight to the bilateral ischium rather than the coccyx. Patients who present with acute or chronic coccygodynia will sit leaning toward one side and not even be aw aie that they are doing this. They will shift their body weight onto one ischial tuberosity, allowing for less pressure on the coccyx. Prolonged and repeated side leaning may lead to shortening of the quadratus lumborum, TFL, psoas, iliacus, or piriformis, along with ischial bursitis, all in addition to coccyxarea pain (coccygodynia).
Dr. Jeffrey Tucker is the 2012 ACA Rehab Council Doctor of the Year. He is also on the education committee for the Hygenic Corporation, and is a post-graduate instructor for the diplomate program offered by the American Chiropractic Rehabilitation Board. Visit his website at www.DrJeffreyTucker.com