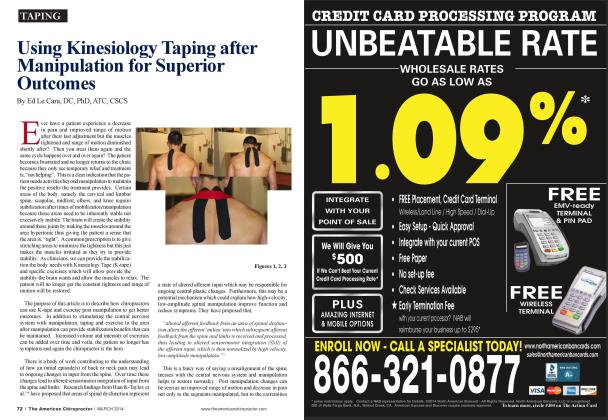
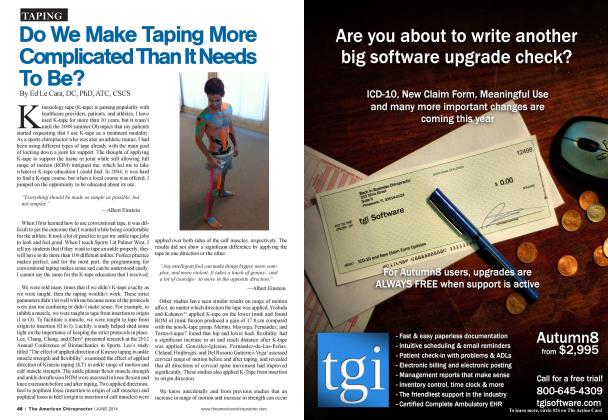
I TEACH CONTINUING EDUCATION FOR CHIROPRACTORS. ATHLETIC TRAINERS. PHYSICAL THERAPISTS. MASSAGE THERAPISTS. AND OTHER ALLIED HEALTH CARE PROVIDERS ALL OVER THE WORLD. WHEN I AM STANDING ON MY SOAPBOX ABOUT THE IMPORTANCE OF HOME EXERCISE. THE COMMON QUESTIONS ASKED ARE HOW AND WHAT TO PRESCRIBE. Start with the assessment After I have ruled out any red flags or need for diagnostics. I go to my whole body assessment. As you can see at the base of Figure 1. the assessment is the foundation of my musculo-skclctal treatment. I dont want to waste my patients" time with an extended regimen of soft tissue therapy if the soft tissue is not the problem. During the assessment. I try to determine if the primary problem is joint, soft tissue, or neurological (motor control). Although all three of these overlap. I can determine the primary problem and use that as a starting point. Detennine the patient's biggest problem and start from there. Based on this assessment is how I direct my care in the office and home. You sec. home care doesn't change what I do in the office. If you look at Figure 1 again, you sec that after the initial assessment I go to joint manipulation (if needed), then to soft tissue, and then to exercise (motor control). The goal of the home exercise is to get the patient involved in their healthcare and extend the care I provided. For example, if I feel the primary problem is joint restriction. I will prescribe banded distractions for the patient to do at home (sec Figure 3 for a banded mobilization of the hip joint). I would prescribe this type of exercise twice per day for between 10 to 20 repetitions. Win so frequent? Soft tissue wont change by treating it every other day. Soft tissue requires constant stress to reorganize. Because of the regularity of this type of exercise. I would add a stretch in conjunction with this mobility. If we overload the patient with too many exercises, he or she just wont be as compliant. The maximum I will prescribe is 2 exercises in a session. If the problem is soft tissue. I would prescribe soft tissue manipulation using a foam roll or using a ball. Continuing with the hip example. I may have the patient use a lacrosse ball in the glutc while they perform internal and external rotation of the hip. I would then follow that exercise with a stretch of the soft tissue structures. Lastly, if the patient has a motor control problem. I would prescribe some exercises that bring awareness to the brain in regard to the area. My goal here would be to recruit more motor units and groove a movement pattern. For example, the hip may have been restricted but the restriction is inconsistent. This means that while the person is standing or sitting he or she may have restriction, but if he or she is lying down the restriction immediately disappears. Therefore, the soft tissue or joint is not truly shortened or compromised, but the body docs not allow the movement in a weight-bearing posture. Essentially, the brain is scared to allow the person too much movement because it thinks that too much movement will lead to tissue injury. I sec this reaction in the hamstrings a lot. You ask patients to touch their toes and they can"t because they, "have had tight hamstrings their whole life": but when you put them in a seated position, they can touch their toes. The inconsistency from standing to sitting is a clear indication the soft tissue is not truly shortened. You could have the patient foam roll, stretch, mash, crash, whatever to the hamstring but nothing will change. Prescribe motor control exercises to the core and hamstring and you will sec change rapidly. The patient will be able to touch his or her toes for the first time and think you perform miracles. Although I just touched on some basic philosophies of what exercises to prescribe, using your clinical skills to determine the underlying cause of the problem the patient is presenting with will provide better outcomes and have the patient giving you rave reviews. Getting the patient involved with proper home exercise programs will differentiate you from a lot of other providers out there and get the patient better, faster. Ed Le Cara, DC, PhD, ATC, CSCS is board certified in sports medicine and rehabilitation. He is a chiropractic clinician, educator and on the medical advisory board for Rocktape. lie provides live and online education for movement professionals at www. HealthandliellnessProviders.com. To contact him, email at drlecarafSiSportsPlusBayArea.com or follow on Twitter: @ drlecara. He hosts a monthly webinar demonstrating different taping applications and answers questions. Look on Google Hangouts under 'Basics ofKinesiology Taping'for his next event.