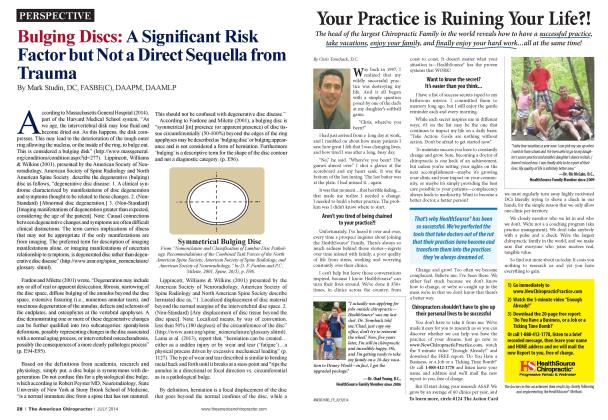
(aka Left Herniation and Right Side Pain) I t is not uncommon for a patient who reports spine-related pain on one side only to have clinical findings and pathology on the side opposite of the pain. When studying the etiology of the contralateral pain in the vertebral column, it is important to understand and consider the osseous and neural anatomy, biomechanics, and related ligamentous attachments responsible for mobility, stability, and load bearing of the spinal unit as a whole. In addition, it is crucial to understand that the vertebral column is a closed fluid system that is sensitive to space-occupying lesions, which can alter pressures based upon displaced fluid. The topic of ipsilatcral lesions with contralatcral pain has been associated with hypertrophy of ligamenta flava. central inncn atioa tractioa and comprcssivc forces. These types of forces have all been associated with space-occupying lesions (hcrniatcd discs) and commented on in the literature. Suca and Gelal (2006) reported. "In our scries, we chose to approach only through the hcrniation side without intervention to the contralatcral symptomatic side. Resolution of symptoms and signs in all of our patients after operation proves that lumbar disk hcrniations can cause dominantly contralatcral symptoms, and that our approach is sufficient and intervention to the contralatcral side is unnecessary "(p. 573). In additioa the authors continued, "...that the contralatcral findings may be related to traction forces rather than contact forces. When the projection of the apex is at the midpoint of the base of a para-median disk herniation (symmetric disk hcrniation). the traction generated on both nerve roots is expected to be equal...However, when the apex of hcrniation is deviated laterally (laterally skewed disk herniation). the traction generated on the contralateral nerve root is expected to be more than that on the ipsilatcral nerve root" (Suca & Gclal. 2006. p. 574). "Our study clearly shows that sciatica can be caused by contralateral lumbar disk hcrniation. When operation is considered, intervention only from the hcrniation side is sufficient. It is probable that traction rather than direct compression is responsible for the emergence of contralatcral symptoms" (Suca & Gclal. 2006. p. 574). Karabckirct al. (2010) reported, "...we have suggested that the ipsilatcral nerve root and dural sac may be displaced posteriorly and laterally towards the contralatcral foramina without significant compression, but the opposite side nerve root is compressed between the facet and hypertrophied ligamenta flava in the lateral recess. Nakagawa ct al. reported two disc hcrniation cases with contralatcral symptoms and their endoscopic surgical observation revealed inflammatory findings of the nerve root on the symptomatic side, such as fibrosis. adhesion and swelling, but the ipsilatcral asymptomatic disc hcrniatcd side did not demonstrate any findings of inflammation or compression...our results indicate that sciatica with contralatcral disc hcrniation may be related to hypertrophied and asymmetrical ligamenta flava..." (p. 621). Hirayama ct al. (2006) reported "...the possible sources of low -back pain caused by lumbar disc hcrniation arc the dorsal ramus component of an injured nerve root.. .the lumbar disc itself.. .and compressed dura...Although it is probable that the dorsal ramus component of an injured nerve root may cause unilateral low-back pain, the lumbar disc and dura are innervated bilaterally... .which may affect PPTs [pressure pain thresholds] on both sides" (p. 45). "One possible explanation is hypcrsensitivity of the sensory neurons of an injured dorsal ramus caused by lumbar disc hcrniation. It has been reported that injured sensory neurons frequently become electrically hypcrcxcitablc due to uprcgulation of voltagc-dcpcndcnt ion channels.... which may partly contribute to the hypcralgcsia in the animal model. The presence of a "tendcrpoint.' usually noticed around the sciatic nerve in patients with lumbar disc hcrniation. is well known...However, the area where decreased PPTs were found was not restricted only to the area innervated by the injured dorsal ramus of L5 or SI nerve root" (Hirayama ct al.. 2006. p. 46). "It has been reported that a barrage of nociccptivc input results in changes to the response properties of dorsal horn neurons and amplifies other noxious or non-noxious inputs...It was reported that experimentally induced muscle pain lowers pain threshold in an area distant to the pain induction in humans...Furthermore, in animal studies, expansion of receptive fields of the deep structures, as well as receptive fields of the skin, lias been found as a manifestation of central hyerexcit-ability... Such central processing may explain the lowering of PPTs detected beyond the inncrvation area of the L5 and S1 dorsal ramus in this study.. .The site of lowed PPTs was beyond the inncrvation area of the L5 and SI dorsal ramus. which indicates the involvement of central ncuromcchanisms" (Hirayama et al.. 2006. p. 46). Yi. Kang. Yoon. and Shin (2013) stated, "...contralatcral complete L5 palsy following ipsilatcral L4 selective transforaminal cpidural block in a patient with central protrusion of the L3-4 intcn crtcbral disc and spinal stenosis with combined disc extrusion to the left lateral recess and lower migration" (p. S56). They went on to further report. "It was suspected that large volumes of fluid injected during neuroplasty could liave caused transient nerve injury from compression within loculated cpidural compartments...The spinal nerve roots may be even more susceptible to compression than peripheral nerves because they arc located in a closed space. In the vertebral column, this means that the canal should be narrowed or the contents increased significantly, as in the case of disc hcrniation" (Yi. Kang. Koon. & Shin. 2013. p. S58). Conclusion: Contralatcral pain from ipsilateral etiology as a hcrniated disc has the follow ing four documented causes: Traction generated from the nerve roots Hypertrophy of asymmetrical liganicnta flava Central hycrcxcitability of the dorsal rami Increased pressure from fluid in a closed spinal region Clinical note: According to the literature and each nonrcfer-enccd study examined to create this review, every conclusion stated that treatment should be limited to the site and side of the lesion where the cause of the contralatcral pain was triggered. The consensus was that treatment on the side of the pain would create complications and elongate the recovery period. References: Suco, II. K.. & Gelal E. (2006) Lumbar disk herniation with con- Iralateral symptoms. European Spine Journal, 15/5): 570 574. Karabekir. II. S.. Yildizhan, A.. Alar. E. A.'.. Yaycioglu. S.. Ciocmen- Slas. A'., & Yazici, C. (2010). Effect oj ligamenlaJ'lava hypertrophy on lumbar disc herniation with contralateral.symptoms and signs: A clinical and morphometric study. Archives of Medical Science. 6(4): 617-622. Hirayama. ./., Yamagala, M., Ogata, S., Shimizu, A", Ikeda, Y., & Takahashi. K. 12006). Relationship between low-back pain, muscle spasm and pressure pain thresholds in patients with lumbar disc hernia tion. European Spine Journal, 15(1): 41-47. Yi. Y.!.. Kang. S. S. Yoon. Y.J.. A Shin. K. M. (2013). Conlralaleral complete 1.5 palsy following ipsi lateral I A selective transforaminal epi- dural block. Korean Journal ofAnesthesiology, 65(6 Suppl), S56-S58. Dr. Mark Studin is an adjunct assistant professor in clinical sciences at the University of Bridgeport College of Chiropractic and a clinical presenter for the State ofXew York at Buffalo, School of Medicine and Biomedical Sciences for post-doctoral educa- lion, leaching MM spine interpretation and tri aging trauma cases. He is also the president of the Academy of Chiropractic teaching doctors of chiropractic how to interface with the legal community (www.LmvversPIProgram.com) and teaches AIR1 interpretation and triaging trauma cases to doctors of all disciplines nationally (www.TeachDoctors.com). He can be reached at DrMark'a'TeachDoctors.com or at 631-786-4253.