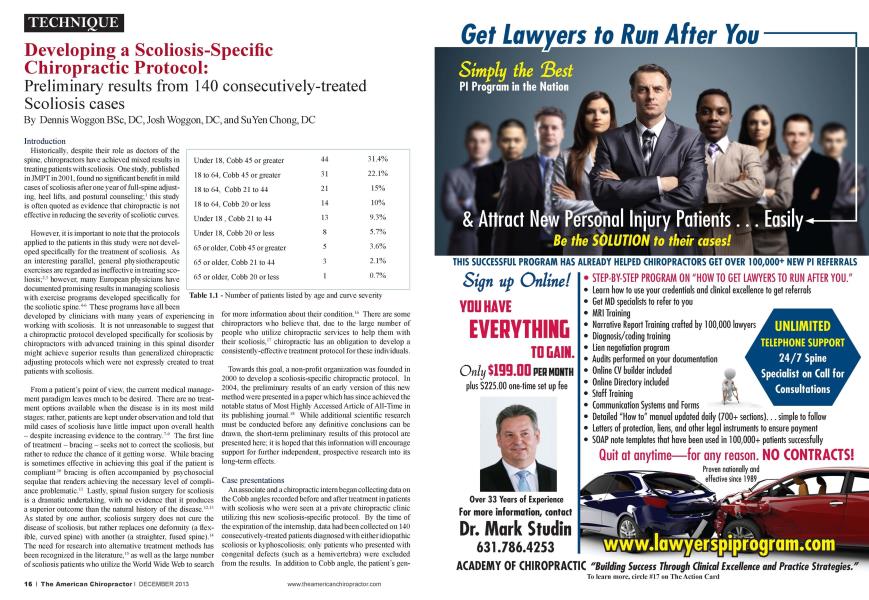
Introduction Historically, despite their role as doctors of the spine, chiropractors have achieved mixed results in treating patients with scoliosis. One study, published in JMPT in 2001. found no significant benefit in mild cases of scoliosis after one year of full-spine adjusting, heel lifts, and postural counseling;1 this study is often quoted as evidence that chiropractic is not effective in reducing the severity of scoliotic curves. However, it is important to note that the protocols applied to the patients in this study were not developed specifically for the treatment of scoliosis. As an interesting parallel, general physiothcrapcutic exercises arc regarded as ineffective in treating scoliosis:2' however, many European physicians have documented promising results in managing scoliosis with exercise programs developed specifically for the scoliotic spine.4"'' These programs have all been developed by clinicians with many years of experiencing in working with scoliosis. It is not unreasonable to suggest that a chiropractic protocol developed specifically for scoliosis by chiropractors with advanced training in this spinal disorder might achieve superior results than generalized chiropractic adjusting protocols which were not expressly created to treat patients with scoliosis. From a patient's point of view, the current medical management paradigm leaves much to be desired. There arc no treatment options available when the disease is in its most mild stages: rather, patients arc kept under observation and told that mild cases of scoliosis have little impact upon overall health - despite increasing evidence to the contrary.""1' The first line of treatment - bracing - seeks not to correct the scoliosis. but rather to reduce the chance of it getting worse. While bracing is sometimes effective in achieving this goal if the patient is compliant"' bracing is often accompanied by psychosocial scqulac that renders achieving the necessary level of compliance problematic." Lastly, spinal fusion surgery for scoliosis is a dramatic undertaking, with no evidence that it produces a superior outcome than the natural history of the disease.12" As stated by one author, scoliosis surgery docs not cure the disease of scoliosis. but rather replaces one deformity (a flexible, curved spine) with another (a straighten fused spine).14 The need for research into alternative treatment methods has been recognized in the literature.15 as well as the large number of scoliosis patients who utilize the World Wide Web to search for more information about their condition."' There are some chiropractors who believe that, due to the large number of people who utilize chiropractic sen ices to help them with their scoliosis.1' chiropractic las an obligation to develop a consistently-effective treatment protocol for these individuals. Towards this goal, a non-profit organization was founded in 2000 to develop a scoliosis-spccific chiropractic protocol. In 2004. the preliminary results of an early version of this new method were presented in a paper which lias since achieved the notable status of Most Highly Accessed Article of Ail-Time in its publishing journal.18 While additional scientific research must be conducted before any definitive conclusions can be drawn, the short-term preliminary results of this protocol arc presented here: it is hoped that this information will encourage support for further independent, prospective research into its long-term effects. Case presentations An associate and a chiropractic intern began collecting data on the Cobb angles recorded before and after treatment in patients with scoliosis who were seen at a private chiropractic clinic utilizing this new scoliosis-spccific protocol. By the time of the expiration of the internship, data had been collected on 140 consecutively-treated patients diagnosed with cither idiopathic scoliosis or kyphoscoliosis: only patients who presented with congenital defects (such as a hemivcrtcbra) were excluded from the results. In addition to Cobb angle, the patient's gen- dcr. age. curve pattern, and number of visits were also recorded. Out of 140 patients. 115 were female. Ill had right primary thoracic curves. 25 had left primary thoracic curves, and 4 had primary lumbar curves with no thoracic component. The collected data was subdivided into categories based upon patient age (under 18; between 18 to 64: or. 65 and older) and curve severity (20 degrees or below; between 21 to 44 degrees: or. 45 degrees and greater). The greatest number of patients (44. representing nearly one-third of all patients seen) were under 18 with Cobb angles of 45 degrees or greater. The average amount of reduction in Cobb angle was 37.7%. Patients with Cobb angles under than 20 degrees experienced the highest average Cobb angle reductions. Treatment Protocol The patients in this study were treated with a protocol developed specifically for the treatment of scoliosis. informally termed Mix. Fix. and Set™, which at the time included active spinal mobility exercises: traction: passive vibration therapy: flexion-distraction therapy: manual, drop-assisted, and instrument-assisted adjusting: whole-body vibration therapy; spinal isometric exercises: and. spinal weighting. Since this data was collected, the protocol has evoked to include additional components, such as therapies designed specifically for ncuro-muscular re-education. Discussion According to the primary treating doctor, the most common reason that patients under 18 years of age with Cobb angles 45 degrees or greater sought care was to avoid surgery, while patients over 18 tended to express a desire to improve their health-related quality of life. The fact that the majority of patients presented for care with Cobb angles of 45 degrees or greater rellects the point of view that many of them did not seek out alternative treatment options until they were confronted with the decision to undergo surgery. One important point to consider is the fact that, due to the rotation of the spine on a radiograph. Cobb angle is not a linear measurement (e.g.. a Cobb angle of 60 degrees is more than twice as severe as a Cobb angle of 30 degrees).19 This may account for the fact that more severe cases appeared to experience a smaller Cobb angle reduction. While the long-term results were not recorded, clinical observations suggest that continued treatment - the extent of which must be determined on a case-by-case basis - is necessary to maintain the results: in the absence of any follow-up care, it is likely that the scoliosis can resume progressing, particularly in Cobb angles greater than 30 degrees. The tenets of evidence-based medicine encourage innovation in areas where it is needed. The current guidelines for conservative management of scoliosis do not include chiropractic management.-" as there is insufficient scientific evidence from which to draw conclusions regarding the effectiveness of chiropractic scoliosis treatment. This is not a rarity in healthcare: nearly one-half of all medical interventions currently in use today lack sufficient evidence to justify their use.-1 When the scientific evidence is lacking, cvidcncc-bascd principles place a high value on the expertise and past experience of the individual clinician, as well as the preferences of the patient. All of the patients in this article self-selected a scoliosis-specific chiropractic protocol as their treatment of choice. Conclusion Certain Haws occurred in data collection which prevented the publication of this data in a pccr-rcvicwcd. scientific article. Nevertheless, this anecdotal evidence suggests that a scoliosis-specific chiropractic protocol may be able to achieve consistently positive results in a wide variety of cases. Considering the public perception of chiropractors as doctors of the spine and the frequency with which people with scoliosis visit chiropractors, investing the resources of our profession into developing an effective treatment regimen and documenting its results scientifically should be considered a necessary goal over the coming years. The authors would like to express their appreciation to Kristin Gulliver DC for her assistance with data collection. ^ To view references go to page 68 Dr. Dennis Woggon is the founder of the CLEAR Scoliosis Institute and the St. Cloud C ^hiropraclic Clinic. He graduated from Palmer College of Chiropractic in 1974. He is an international instructor for CLEAR Scoliosis Institute. He can be contacted at dnvoggonklclear-institute.org. Dr. A. Joshua Woggon, a 2010 Graduate of Parker College, serves as the Director of Research for the CLEAR Scoliosis Institute, a Non-Profit Organization dedicated to advancing chiropractic scoliosis correc- lion (www.clear-in.sliliile.org). He can be contacted at jwoggon(a,clear-inslilule.org. Dr. SuYen Chong is a 2005 Palmer College of Chiropractic Alumni with a Doctorate in Chiropractic and a Bachelor of Science degree. She has been an associate at St C loud C liiropraclic C linic and C 1.K-IR Scoliosis Center of Saint Cloud, Minnesota with Dr. Dennis llbggon since July of 2008. She can be contacted at drsuyencliong<ci clear-instilute.org. ► (\mtinued from page 22 References Lain/ CA. Chen J: Effect of chiropractic intervention on small scoliotic curves in younger subjects: a time-series cohort design. JMPT 2001 Jul-Aug:24(6):385-93. Shands A.R.. Barr J.S.. Colonna PC. Noall L: End-result study of the treatment of idiopalliic scoliosis: report of the Research Committee of the American Orthopedic Association. J Bone Joint Surg. 1941:23-A(4):963-977. Cassclla MC. Hall JE: Current treatment approaches in the non- opcrativc and operative management of adolescent idiopathic scoliosis. Phys Thcr. 1991 Dcc:71(12):897-909. Negrini S. Zaina F. Romano M. Ncgrini A. Par/.ini S: Specific exercises reduce brace prescription in adolescent idiopathic sco liosis: a prospective controlled cohort study with worst-case analysis. J Rchabil Mcd. 2008 Jun:40(6):451-5. Negrini S. Fusco C. Minoz/.i S. Atanasio S. Zaina F. Romano M: Exercises reduce the progression rale of adolescent idiopathic scoliosis: results of a comprehensive systematic review of the literature. Disabil Rchabil. 20()8:30(10):772-85. Weiss HR. Weiss G. Petermann F: Incidence of curvature progres sion in idiopathic scoliosis patients treated with scoliosis in-patient rehabilitation (SIR): an age- and sex-matched controlled study. Pcdialr Rehabil. 2003 Jan-Mar.6(l):23-3O. Barrios C. Pcrez-Encinas C. Mamcnda J.I.. Laguia M: Signifi cant venlilalory functional restriction in adolescents with mild or moderate scoliosis during maximal exercise tolerance test. Spine 2005:30{ 14): 161 ()-1615. DiRocco PJ. Vaccaro P: Cardiopulmonary functioning in ado lescent patients with mild idiopathic scoliosis. Arch Phys Med Rehabil. 1988 Mar:69(3 Pt 1): 198-201. Santos Alvcs VL. Avan/.i O: Objective assessment of the car- diorcspiralory function of adolescents with idiopathic scoliosis through the six-minute walk test. Spine 2009:34(25):E926-E929 Weinslein SL. Dolan LA. Wright JG. Dobbs MB: Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Mcd. 2013 Oct 17:369(16): 1512-21. Ri\ ett L. Rothberg A. Stewart A. Bcrkowitz R: The relationship between quality of life and compliance to a brace protocol in adolescents with idiopathic scoliosis: a comparative study. BMC Musculoskclat Disord. 2009:10:5. Weiss HR. Goodall D: Rate of complications in scoliosis sur gery - a systematic review of the PubMed literature. Scoliosis 2008 Aug 5:3:9. Wcstrick ER. Ward WT: Adolescent idiopathic scoliosis: 5-ycar to 20-ycarcvidcncc-bascd surgical results. J Pcdiatr Orthop. 2011 Jan-Fcb:31(l Suppl):S61-8. Goldberg CJ. Moore DP et al: The effect of brace treatment on the incidence of surgery. Spine 2001.26:42-47. Hawes M. O'Brien J: A century of spine surgery: what can pa tients expect? Disabil Rehabil. 2008:30( 10):808-817. Bcall MS 3rd. Golladay GJ. Greenfield ML. HensingerRN. Bier- mann JS: Use of the Internet by pediatric orthopaedic outpatients. J Pcdiatr Orthop. 2002 Mar-Apr:22(2):261-4. Chrislensen MG. Kerkhoff D. Kollasch MW: Job analysis of chiropractic 2000. Grcclcy. Colorado: National Board of Chi ropractic Examiners: 2000. Morningstar MW. Woggon D. Lawrence G: Scoliosis treatment using a combination of manipulative and rehabilitative therapy: a retrospective case series. BMC Musculoskelet Disord. 2004 Sep 14:5:32. Newton PO ct al: Idiopathic Scoliosis: The Harms Study Group Treatment Guide, p. 20. Negrini et al: 2011 SOSORT guidelines: orthopaedic and re habilitation treatment of idiopathic scoliosis during growth. Scoliosis 2012.7:3. Lew ith G. (cited by Cope J) Heallhw rilcr. April 2007. p 2. data taken from http://clinicalcvidcncc.com/ccw eb/about/ know ledge/ jsp visited 06-05- 07.