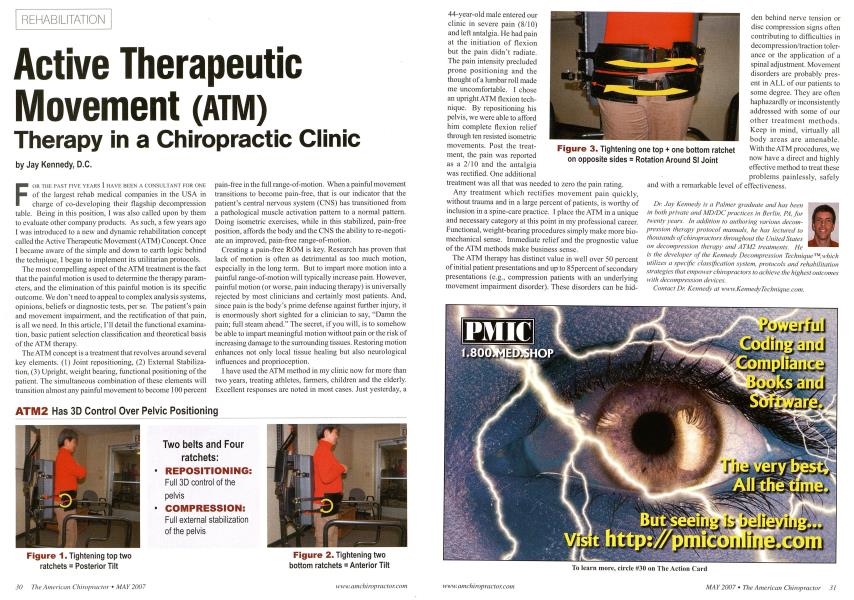
FOR Till- PAST FIVK YEARS I 1IAVH HEEN A CONSULTANT FOR ONE of the largest rehab medical companies in the USA in charge of co-developing their flagship decompression table. Being in this position, I was also called upon by them to evaluate other company products. As such, a few years ago I was introduced to a new and dynamic rehabilitation concept called the Active Therapeutic Movement (ATM) Concept. Once I became aware of the simple and down to earth logic behind the technique, 1 began to implement its utilitarian protocols. The most compelling aspect of the ATM treatment is the fact that the painful motion is used to determine the therapy parameters, and the elimination of this painful motion is its specific outcome. We don't need to appeal to complex analysis systems, opinions, beliefs or diagnostic tests, per se. The patient's pain and movement impairment, and the rectification of that pain, is all we need. In this article, I'll detail the functional examination, basic patient selection classification and theoretical basis of the ATM therapy. The ATM concept is a treatment that revolves around several key elements. (1) Joint repositioning, (2) External Stabilization, (3) Upright, weight bearing, functional positioning of the patient. The simultaneous combination of these elements will transition almost any painful movement to become 100 percent pain-free in the full range-of-motion. When a painful movement transitions to become pain-free, that is our indicator that the patient's central nervous system (CNS) has transitioned from a pathological muscle activation pattern to a normal pattern. Doing isometric exercises, while in this stabilized, pain-free position, affords the body and the CNS the ability to re-negotiate an improved, pain-free range-of-motion. Creating a pain-free ROM is key. Research has proven that lack of motion is often as detrimental as too much motion, especially in the long term. But to impart more motion into a painful range-of-motion will typically increase pain. However, painful motion (or worse, pain inducing therapy) is universally rejected by most clinicians and certainly most patients. And, since pain is the body's prime defense against further injury, it is enormously short sighted for a clinician to say, "Damn the pain; full steam ahead." The secret, if you will, is to somehow be able to impart meaningful motion without pain or the risk of increasing damage to the surrounding tissues. Restoring motion enhances not only local tissue healing but also neurological influences and proprioception. I have used the ATM method in my clinic now for more than two years, treating athletes, fanners, children and the elderly. Excellent responses are noted in most cases. Just yesterday, a ATM2 Has 3D Control Over Pelvic Positioning Two belts and Four ratchets: • REPOSITIONING: Full 3D control of the pelvis • COMPRESSION: Full external stabilization of the pelvis 44-year-old male entered our clinic in severe pain (8/10) and left antalgia. He had pain at the initiation of flexion but the pain didn't radiate. The pain intensity precluded prone positioning and the thought of a lumbar roll made me uncomfortable. I chose an upright ATM flexion technique. By repositioning his pelvis, we were able to afford him complete flexion relief through ten resisted isometric movements. Post the treatment, the pain was reported as a 2/10 and the antalgia was rectified. One additional treatment was all that was needed to zero the pain rating. Any treatment which rectifies movement pain quickly, without trauma and in a large percent of patients, is worthy of inclusion in a spine-care practice. I place the ATM in a unique and necessary category at this point in my professional career. Functional, weight-bearing procedures simply make more bio-mechanical sense. Immediate relief and the prognostic value of the ATM methods make business sense. The ATM therapy has distinct value in well over 50 percent of initial patient presentations and up to 85percent of secondary presentations (e.g., compression patients with an underlying movement impairment disorder). These disorders can be hid- den behind nerve tension or disc compression signs often contributing to difficulties in decompression/traction tolerance or the application of a spinal adjustment. Movement disorders are probably present in ALL of our patients to some degree. They are often haphazardly or inconsistently addressed with some of our other treatment methods. Keep in mind, virtually all body areas are amenable. With the ATM procedures, we now have a direct and highly effective method to treat these problems painlessly, safely and with a remarkable level of effectiveness. Dr. Jav Kennedy is a Palmer graduate and has been in both private and MD/DC practices in Berlin, PA, for twenty years. In addition to authoring various decompression therapy protocol manuals, he has lectured to thousands of chiropractors throughout the United States on decompression therapy and ATM- treatments. He is the developer of the Kennedy Decompression Technique™,\vhich utilizes a specific classification system, protocols and rehabilitation strategies that empower chiropractors to achieve the highest outcomes with decompression devices. Contact Dr. Kennedy at www.KennedyTechnique.com. Figure 1. Tightening top two ratchets = Posterior Tilt Figure 2. Tightening two bottom ratchets = Anterior Tilt Figure 3. Tightening one top + one bottom ratchet on opposite sides = Rotation Around SI Joint