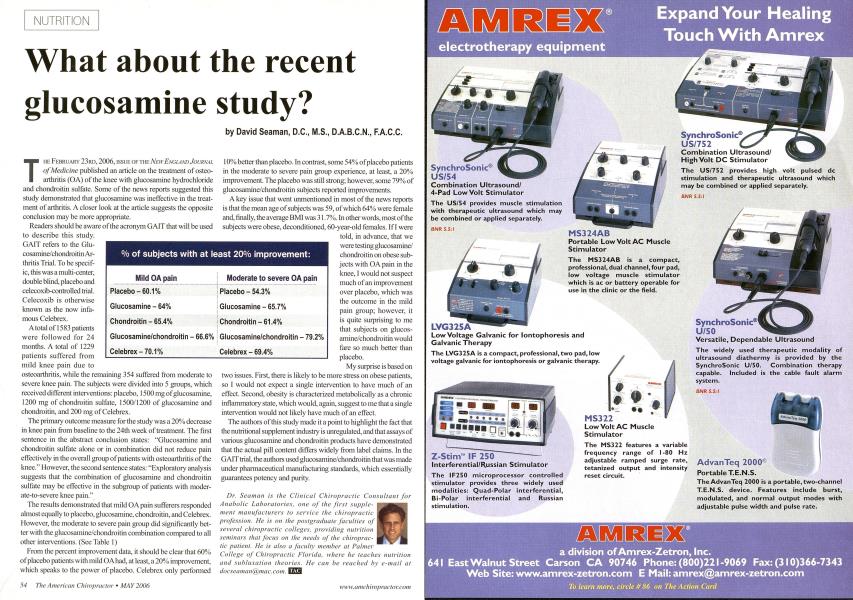
T he February 23rd, 2006, issue of the New England Journal of Medicine published an article on the treatment of osteo-arthritis (OA) of the knee with glucosamine hydrochloride and chondroitin sulfate. Some of the news reports suggested this study demonstrated that glucosamine was ineffective in the treatment of arthritis. A closer look at the article suggests the opposite conclusion may be more appropriate. Readers should be aware of the acronym GAIT that will be used to describe this study. GAIT refers to the Glu-cosamine/chondroitin Arthritis Trial. To be specific, this was a multi-center, double blind, placebo and eeleeoxib-controlled trial. Celecoxib is otherwise known as the now infamous Celebrex. A total of 1583 patients were followed for 24 months. A total of 1229 patients suffered from mild knee pain due to osteoarthritis, while the remaining 354 suffered from moderate to severe knee pain. The subjects were divided into 5 groups, which received different interventions: placebo, 1500 mg of glucosamine, 1200 mg of chondroitin sulfate, 1500/1200 of glucosamine and chondroitin, and 200 mg of Celebrex. The primary outcome measure for the study was a 20% decrease in knee pain from baseline to the 24th week of treatment. The first sentence in the abstract conclusion states: "Glucosamine and chondroitin sulfate alone or in combination did not reduce pain effectively in the overall group of patients with osteoarthritis of the knee." However, the second sentence states: "Exploratory analysis suggests that the combination of glucosamine and chondroitin sulfate may be effective in the subgroup of patients with moderate-to-severe knee pain." The results demonstrated that mild OA pain sufferers responded almost equally to placebo, glucosamine, chondroitin, and Celebrex. However, the moderate to severe pain group did significantly better with the glucosaminc/chondroitin combination compared to all other interventions. (See Table 1) From the percent improvement data, it should be clear that 60% of placebo patients with mild OA had, at least, a 20% improvement, which speaks to the power of placebo. Celebrex only performed 10% better than placebo. In contrast, some 54% of placebo patients in the moderate to severe pain group experience, at least, a 20% improvement. The placebo was still strong; however, some 79% of glucosamine/chondroitin subjects reported improvements. A key issue that went unmentioned in most of the news reports is that the mean age of subjects was 59, of which 64% were female and, finally, the average BMI was 31.7%. In other words, most of the subjects were obese, deconditioned, 60-year-old females. If I were told, in advance, that we were testing gliicosamine/ chondroitin on obese subjects with OA pain in the knee, I would not suspect much of an improvement over placebo, which was the outcome in the mild pain group; however, it is quite surprising to me that subjects on glucos-amine/chondroitin would fare so much better than placebo. My surprise is based on two issues. First, there is likely to be more stress on obese patients, so I would not expect a single intervention to have much of an effect. Second, obesity is characterized metabolically as a chronic inflammatory state, which would, again, suggest to me that a single intervention would not likely have much of an effect. The authors of this study made it a point to highlight the fact that the nutritional supplement industry is unregulated, and that assays of various glucosamine and cliondroitin products have demonstrated that the actual pill content differs widely from label claims. In the GAIT trial, the authors used glucosamine/chondroitin that was made under pharmaceutical manufacturing standards, which essentially guarantees potency and purity. Dr. Seaman is the Clinical Chiropractic Consultant for Anabolic Laboratories, one of the first supplement manufacturers to service the chiropractic profession. He is on the postgraduate faculties of several chiropractic colleges, providing nutrition seminars that focus on the needs of the chiropractic patient. He is also a faculty member at Palmer College of Chiropractic Florida, where he teaches nutrition anil subliixation theories. He can be reached bv e-mail at [email protected]. I