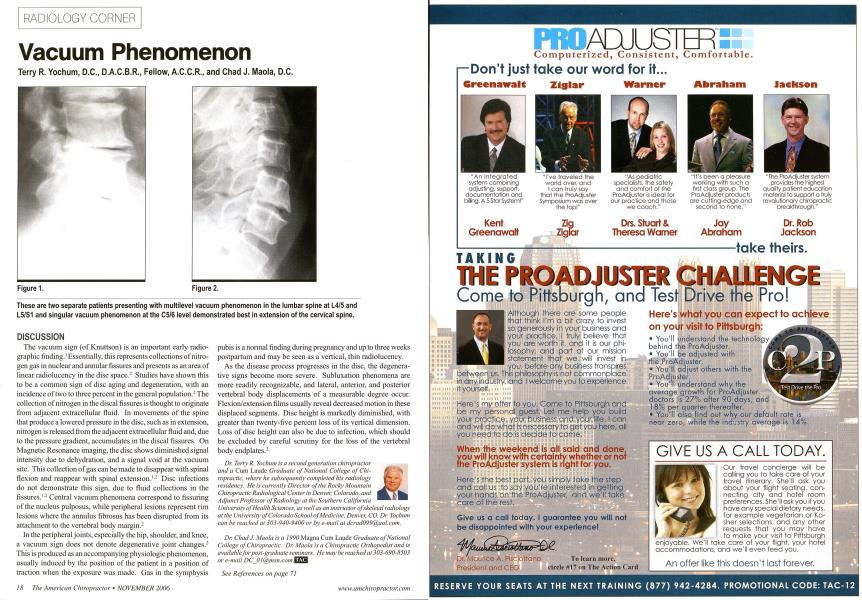
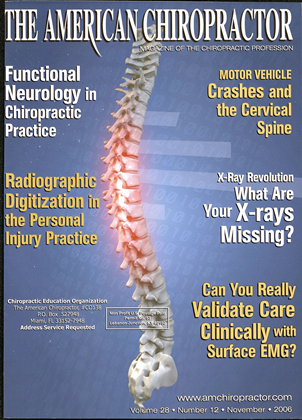
Terry R. Yochum, D.C., D.A.C.B.R., Fellow, A.C.C.R., and Chad J. Maola, D.C. DISCUSSION The vacuum sign (of Knuttson) is an important early radio-graphic finding.1 Essentially, this represents collections of nitrogen gas in nuclear and annular fissures and presents as an area of linear radiolucency in the disc space.2 Studies have shown this to be a common sign of disc aging and degeneration, with an incidence of two to three percent in the general population.2 The collection of nitrogen in the discal fissures is thought to originate from adjacent extracellular fluid. In movements of the spine that produce a lowered pressure in the disc, such as in extension, nitrogen is released from the adjacent extracellular fluid and, due to the pressure gradient, accumulates in the discal fissures. On Magnetic Resonance imaging, the disc shows diminished signal intensity due to dehydration, and a signal void at the vacuum site. This collection of gas can be made to disappear with spinal flexion and reappear with spinal extension.1-2 Disc infections do not demonstrate this sign, due to fluid collections in the fissures.'- Central vacuum phenomena correspond to fissuring of the nucleus pulposus, while peripheral lesions represent rim lesions where the annulus fibrosus has been disrupted from its attachment to the vertebral body margin.2 In the peripheral joints, especially the hip, shoulder, and knee, a vacuum sign does not denote degenerative joint changes.2 This is produced as an accompanying physiologic phenomenon, usually induced by the position of the patient in a position of traction when the exposure was made. Gas in the symphysis pubis is a normal finding during pregnancy and up to three weeks postparrum and may be seen as a vertical, thin radiolucency. As the disease process progresses in the disc, the degenerative signs become more severe. Subluxation phenomena are more readily recognizable, and lateral, anterior, and posterior vertebral body displacements of a measurable degree occur. Flexion/extension films usually reveal decreased motion in these displaced segments. Disc height is markedly diminished, with greater than twenty-five percent loss of its vertical dimension. Loss of disc height can also be due to infection, which should be excluded by careful scrutiny for the loss of the vertebral body endplates.2 Dr. TenyR. Yochum is a second generation chiropractor and a Cum Laude Graduate of National College of Chiropractic, where he subsequently completed his radiology residency. He is currently Director of the Rocky Mountain Chiropractic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology at the Southern California University of Health Sciences, as well as an instructor of skeletal radiolog}' at the University of Colorado School of Medicine, Denver, CO. Dr. Yochum can be reached at 303-940-9400 or by e-mail at [email protected]. Dr. ChadJ. Maola is a 1990 Magna Cum Laude Graduate of National College of Chiropractic. Dr. Maola is a Chiropractic Orthopedist and is available for post-graduate seminars. He may be reached at 303-690-8503 or e-mail [email protected] See References on page 71 Figure 1. Figure 2. These are two separate patients presenting with multilevel vacuum phenomenon in the lumbar spine at L4/5 and L5/S1 and singular vacuum phenomenon at the C5/6 level demonstrated best in extension of the cervical spine.