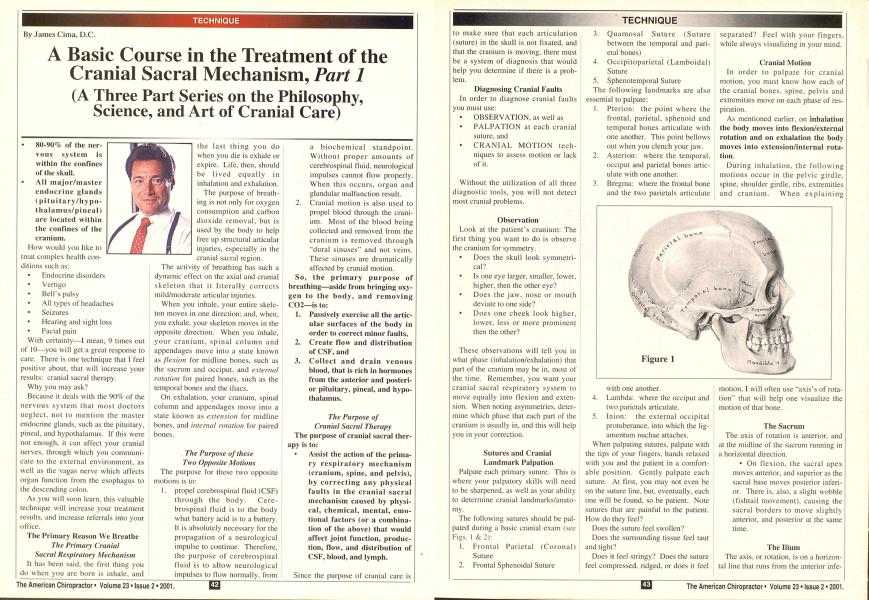
80-90% of the ner vous system is within the confines of the skull. All major/master endocrine glands (pituitary/hypo- thalamus/pineal) are located within the confines of the cranium. How would you like to treat complex health con- ditions such as: Endocrine disorders Vertigo BelTs palsy All types of headaches Seizures Hearing and sight loss Facial pain With certainty—I mean, 9 times out of 10—you will get a great response to care. There is one technique that I feel positive about, that will increase your results: cranial sacral therapy. Why you may ask? Because it deals with the 90% of the nervous system that most doctors neglect, not to mention the master endocrine glands, such as the pituitary, pineal, and hypothalamus. If this were not enough, it can affect your cranial nerves, through which you communicate to the external environment, as well as the vagas nerve which affects organ function from the esophagus to the descending colon. As you will soon learn, this valuable technique will increase your treatment results, and increase referrals into your office. The Primary Reason We Breathe The Primary Cranial Sacral Respiratory Mechanism It has been said, the first thing you do when you are born is inhale, and the last thing you do when you die is exhale or expire. Life, then, should be lived equally in inhalation and exhalation. The purpose of breathing is not only for oxygen consumption and carbon dioxide removal, but is used by the body to help free up structural articular injuries, especially in the cranial sacral region. The activity of breathing has such a dynamic effect on the axial and cranial skeleton that it literally corrects mild/moderate articular injuries. When you inhale, your entire skeleton moves in one direction; and, when, you exhale, your skeleton moves in the opposite direction. When you inhale, your cranium, spinal column and appendages move into a state known as flexion for midline bones, such as the sacrum and occiput, and external rotation for paired bones, such as the temporal bones and the iliacs. On exhalation, your cranium, spinal column and appendages move into a stale known as extension for midline bones, and internal rotation for paired bones. The Purpose of these Two Opposite Motions The purpose for these two opposite motions is to: 1. propel cerebrospinal fluid (CSF) through the body. Cerebrospinal fluid is to the body what battery acid is to a battery. It is absolutely necessary for the propagation of a neurological impulse to continue. Therefore, the purpose of cerebrospinal fluid is to allow neurological impulses to How normally, from a biochemical standpoint. Without proper amounts of cerebrospinal fluid, neurological impulses cannot flow properly. When this occurs, organ and glandular malfunction result. 2. Cranial motion is also used to propel blood through the cranium. Most of the blood being collected and removed from the cranium is removed through "dural sinuses" and not veins. These sinuses are dramatically affected by cranial motion. So, the primary purpose of breathing—aside from bringing oxygen to the body, and removing CO2—is to: Passively exercise all the artic ular surfaces of the body in order to correct minor faults, Create flow and distribution of CSF, and Collect and drain venous blood, that is rich in hormones from the anterior and posteri or pituitary, pineal, and hypo- thalamus. The Purpose of Cranial Sacral Therapy The purpose of cranial sacral therapy is to: • Assist the action of the primary respiratory mechanism (cranium, spine, and pelvis), by correcting any physical faults in the cranial sacral mechanism caused by physical, chemical, mental, emotional factors (or a combination of the above) that would affect joint function, production, How, and distribution of CSF, blood, and lymph. Since the purpose of cranial care is to make sure that each articulation (suture) in the skull is not fixated, and that the cranium is moving, there must be a system of diagnosis that would help you determine if there is a problem. Diagnosing Cranial Faults In order to diagnose cranial faults you must use: OBSERVATION, as well as PALPATION at each cranial suture, and CRANIAL MOTION tech niques to assess motion or lack of it. Without the utilization of all three diagnostic tools, you will not detect most cranial problems. Observation Look at the patient's cranium: The first thing you want to do is observe the cranium for symmetry. Does the skull look symmetri cal? Is one eye larger, smaller, lower, higher, then the other eye? Does the jaw, nose or mouth deviate to one side? Does one cheek look higher, lower, less or more prominent then the other? These observations will tell you in what phase (inhalation/exhalation) that part of the cranium may be in, most of the time. Remember, you want your cranial sacral respiratory system to move equally into flexion and extension. When noting asymmetries, determine which phase that each part of the cranium is usually in. and this will help you in your correction. Sutures and Cranial Landmark Palpation Palpate each primary suture. This is where your palpatory skills will need to be sharpened, as well as your ability to determine cranial landmarks/anatomy. The following sutures should be palpated during a basic cranial exam (see Figs. I & 2): Frontal Parietal (Coronal) Suture Frontal Sphenoidal Suture Quamosal Suture (Suture between the temporal and pari etal bones) Occipitoparietal (Lamboidal) Suture Sphenotemporal Suture The following landmarks are also essential to palpate: Pterion: the point where the frontal, parietal, sphenoid and temporal bones articulate with one another. This point bellows out when you clench your jaw. Asterion: where the temporal, occiput and parietal bones artic ulate with one another. Bregma: where the frontal bone and the two parietals articulate with one another. Lambda: where the occiput and two parietals articulate. Inion: the external occipital protuberance, into which the lig- amentum nuchae attaches. When palpating sutures, palpate with the tips of your fingers, hands relaxed with you and the patient in a comfortable position. Gently palpate each suture. At first, you may not even be on the suture line. but. eventually, each one will be found, so be patient. Note sutures that are painful to the patient. How do they feel? Does the suture feel swollen? Does the surrounding tissue feel taut and tight? Does it feel stringy? Does the suture feel compressed, ridged, or does it feel separated? Feel with your fingers, while always visualizing in your mind. Cranial Motion In order to palpate for cranial motion, you must know how each of the cranial bones, spine, pelvis and extremities move on each phase of respiration. As mentioned earlier, on inhalation the body moves into flexion/external rotation and on exhalation the body moves into extension/internal rotation. During inhalation, the following motions occur in the pelvic girdle, spine, shoulder girdle, ribs, extremities and cranium. When explaining motion. I will often use "axis's of rotation" that will help one visualize the motion of that bone. The Sacrum The axis of rotation is anterior, and at the midline of the sacrum running in a horizontal direction. • On flexion, the sacral apex moves anterior, and superior as the sacral base moves posterior inferior. There is. also, a slight wobble (fishtail movement), causing the sacral borders to move slightly anterior, and posterior at the same time. The Ilium The axis, or rotation, is on a horizontal line that runs from the anterior infe- rior spine of the ilium to the greater , sacrosciatic notch. | The ilium moves into external rota- j tion on inhalation, because they are i paired bones. • On inhalation, the anterior ; superior iliac spine moves superi- | or, and laterally, while the posteri- j or superior iliac spine moves infe- i rior and medially. This motion is I easy to detect with the patient in a I prone position. Take your linger- j tips and position them under the | anterior superior iliac spines and j have the patient inhale. As the j patient inhales, the anterior superi- j or iliac spine moves away from j your linger tips. I This motion of the ilium causes j external rotation of the femur, tibia/fibulur articulations, which Hare i out both ankles and feet, bringing them i into external rotation. 1 | The Spine ; On inhalation, the spine shortens j from its superior inferior direction and, I at the same time, the lordotic, and I kyphotic (anterior and posterior [ curves) increase, becoming more j hyperlordotic and kyphotic. 1 The Ribs ! On inhalation, the ribs move anteri- j orly, laterally, and superiorly, greatly j affecting the shoulder girdle, moving j the upper extremities, elbows, and j wrists into external rotation, which supinutes the palms of your arms and | hands. I The Cranium j On inhalation, the cranium widens \ laterally and decreases in its anterior- j to-posterior dimensions. The land- j marks used to determine the anterior- I to-posterior dimension is from the j external occipital protuberance, to the I glabella. j The Sphenobasilar Mechanism ; (The main hub for ! all cranial motion) \ The sphenobasilar mechanism is j composed of the basilar portion of the j occiput, and the basilar portion of the i sphenoid. This is a cartilaginous ; union, which gives it a slight bending ; motion. During flexion, this cartilagi- ■ nous union bends or Ilexes in a superior direction. This mechanism, then, as mentioned earlier, activates and drives all cranial motion (a main hub). Since every cranial bone articulates with the sphenoid, the sphenoid then sets into motion the rest of the cranium. Therefore, to some degree, most cranial motion rests on the integrity of the sphenobasilar mechanism. Making sure that this mechanism is moving properly is an absolute must for cranial motion. The occiput moves as the sacrum does. The temporals, being paired bones, follow a similar motion to that of the iliac bones. Just as the sacrum is | sandwiched between the ilia, the I occiput is sandwiched between the ! temporal bones. 1 When the sacral apex moves anterior j and superior on flexion, the anterior | aspect of the foramen magnum moves I anterior superior, as the squamosal I portion of the occiput moves inferior. Just as the ilia move in a posterior superior direction at the anterior supe rior iliac spines, the temporals move in | a posterior, superior direction at the i temporal squama. | The frontal moves anterior inferior I a( the frontal eminence, by the action of the sphenoid, as the parietals compensate by rocking back and forth. The motion in the cranium can become very complex and, for a more in-depth discussion, please refer to my book j entitled The Cranial Concept. In this book, each cranial bone is discussed in great length, with much more detail. For now, I would just like you to get your feet and appetite wet for more knowledge. Then, as we delve further into cranial work, you will have a foundation to build from. In Part 2 of this series, I will explain how to go about evaluating cranial problems, using breathing and palpation. These techniques will not only help you diagnosis and find the cranial faults, but help you in the correction of basic cranial conditions. In Part 3, I will cover the basic contacts necessary when treating basic cranial faults. Until the next article, review this article, and begin palpating and finding as many of these sutures/landmarks on your patients as you can. If you have a real skull or a plastic model, palpate and feel the sutures of the real skull or model. You will be surprised at how close these sutures and landmarks feel to the real thing. Until next time may your practice and health nourish. Dr. James Cima has been teaching, and writing on this subject for 20 years. Dr. Cima also teaches seminars and has created a software package for the doctors to help them assess their patients' needs. For more information, call toll free 1-877-627-2770 or fax 561-624-3871, or e-mail Dr. Cima at [email protected]. o